

The hypoxic burden of sleep apnoea predicts cardiovascular disease-related mortality: the Osteoporotic Fractures in Men Study and the Sleep Heart Health Study
- PMID: 30376054
- PMCID: PMC6451769
- DOI: 10.1093/eurheartj/ehy624
The hypoxic burden of sleep apnoea predicts cardiovascular disease-related mortality: the Osteoporotic Fractures in Men Study and the Sleep Heart Health Study
Erratum in
-
Corrigendum to: The hypoxic burden of sleep apnoea predicts cardiovascular disease-related mortality: the Osteoporotic Fractures in Men Study and the Sleep Heart Health Study.Eur Heart J. 2019 Apr 7;40(14):1157. doi: 10.1093/eurheartj/ehz028. Eur Heart J. 2019. PMID: 30753451 Free PMC article. No abstract available.
Abstract
Aims: Apnoea-hypopnoea index (AHI), the universal clinical metric of sleep apnoea severity, poorly predicts the adverse outcomes of sleep apnoea, potentially because the AHI, a frequency measure, does not adequately capture disease burden. Therefore, we sought to evaluate whether quantifying the severity of sleep apnoea by the 'hypoxic burden' would predict mortality among adults aged 40 and older.
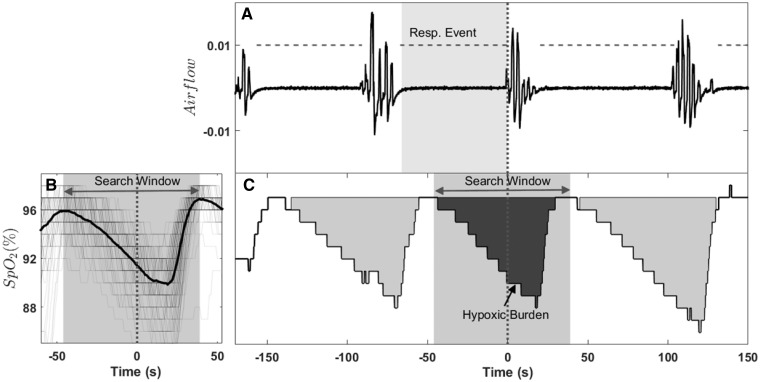
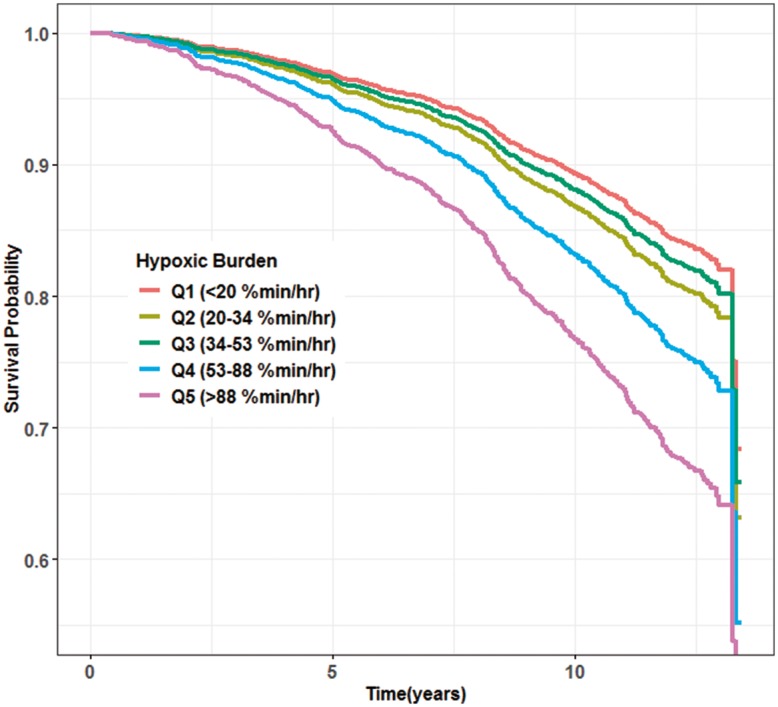
Methods and results: The samples were derived from two cohort studies: The Outcomes of Sleep Disorders in Older Men (MrOS), which included 2743 men, age 76.3 ± 5.5 years; and the Sleep Heart Health Study (SHHS), which included 5111 middle-aged and older adults (52.8% women), age: 63.7 ± 10.9 years. The outcomes were all-cause and Cardiovascular disease (CVD)-related mortality. The hypoxic burden was determined by measuring the respiratory event-associated area under the desaturation curve from pre-event baseline. Cox models were used to calculate the adjusted hazard ratios for hypoxic burden. Unlike the AHI, the hypoxic burden strongly predicted CVD mortality and all-cause mortality (only in MrOS). Individuals in the MrOS study with hypoxic burden in the highest two quintiles had hazard ratios of 1.81 [95% confidence interval (CI) 1.25-2.62] and 2.73 (95% CI 1.71-4.36), respectively. Similarly, the group in the SHHS with hypoxic burden in the highest quintile had a hazard ratio of 1.96 (95% CI 1.11-3.43).
Conclusion: The 'hypoxic burden', an easily derived signal from overnight sleep study, predicts CVD mortality across populations. The findings suggest that not only the frequency but the depth and duration of sleep related upper airway obstructions, are important disease characterizing features.
Keywords: Apnoea–hypopnoea index; CVD mortality; Hypoxic burden; Polysomnography; Sleep apnoea.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2018. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
The hypoxic burden: a novel sleep apnoea severity metric and a predictor of cardiovascular mortality-Reply to 'The hypoxic burden: also known as the desaturation severity parameter'.Eur Heart J. 2019 Sep 14;40(35):2994-2995. doi: 10.1093/eurheartj/ehz273. Eur Heart J. 2019. PMID: 31065680 No abstract available.
-
The hypoxic burden: also known as the desaturation severity parameter.Eur Heart J. 2019 Sep 14;40(35):2991-2993. doi: 10.1093/eurheartj/ehz271. Eur Heart J. 2019. PMID: 31065687 No abstract available.
-
How to assess nocturnal hypoxaemic burden in Cardiology?Eur Heart J. 2019 Sep 14;40(35):2988. doi: 10.1093/eurheartj/ehz272. Eur Heart J. 2019. PMID: 31071209 No abstract available.
-
Hypoxic burden captures sleep apnoea-specific nocturnal hypoxaemia.Eur Heart J. 2019 Sep 14;40(35):2989-2990. doi: 10.1093/eurheartj/ehz274. Eur Heart J. 2019. PMID: 31071210 Free PMC article. No abstract available.
References
-
- Young T, Peppard P, Gottlieb D.. The epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med 2002;165:1217–1239. - PubMed
-
- Colt HG, Haas H, Rich GB.. Hypoxemia vs sleep fragmentation as cause of excessive daytime sleepiness in obstructive sleep apnea. Chest 1991;100:1542–1548. - PubMed
-
- White DP, Younes MK.. Obstructive sleep apnea. Compr Physiol 2012;2:2541–2594. - PubMed
-
- Engleman HM, Kingshott RN, Martin SE, Douglas NJ.. Cognitive function in the sleep apnea/hypopnea syndrome (SAHS). Sleep 2000;23(Suppl 4):S102–S108. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 HL071194/HL/NHLBI NIH HHS/United States
- R35 HL135818/HL/NHLBI NIH HHS/United States
- R01 HL070841/HL/NHLBI NIH HHS/United States
- R24 HL114473/HL/NHLBI NIH HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
- U01 AG027810/AG/NIA NIH HHS/United States
- U01 HL053937/HL/NHLBI NIH HHS/United States
- R01 HL070837/HL/NHLBI NIH HHS/United States
- U01 AG042139/AG/NIA NIH HHS/United States
- R01 HL070848/HL/NHLBI NIH HHS/United States
- U01 HL053916/HL/NHLBI NIH HHS/United States
- U01 HL063463/HL/NHLBI NIH HHS/United States
- R01 HL070847/HL/NHLBI NIH HHS/United States
- R01 HL070842/HL/NHLBI NIH HHS/United States
- U01 AG042124/AG/NIA NIH HHS/United States
- U01 AG042145/AG/NIA NIH HHS/United States
- U01 HL053938/HL/NHLBI NIH HHS/United States
- U01 HL053941/HL/NHLBI NIH HHS/United States
- U01 AG042168/AG/NIA NIH HHS/United States
- U01 AG042140/AG/NIA NIH HHS/United States
- R01 HL070838/HL/NHLBI NIH HHS/United States
- U01 HL053934/HL/NHLBI NIH HHS/United States
- U01 HL063429/HL/NHLBI NIH HHS/United States
- R01 HL070839/HL/NHLBI NIH HHS/United States
- UL1 TR001102/TR/NCATS NIH HHS/United States
- U01 AR066160/AR/NIAMS NIH HHS/United States
- U01 HL053931/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
