

Predicting Thromboembolic and Bleeding Event Risk in Patients with Non-Valvular Atrial Fibrillation: A Systematic Review
- PMID: 30376678
- PMCID: PMC6754740
- DOI: 10.1055/s-0038-1675400
Predicting Thromboembolic and Bleeding Event Risk in Patients with Non-Valvular Atrial Fibrillation: A Systematic Review
Abstract
Background: Atrial fibrillation (AF) is a common cardiac arrhythmia that increases the risk of stroke. Medical therapy for decreasing stroke risk involves anticoagulation, which may increase bleeding risk for certain patients. In determining the optimal therapy for stroke prevention for patients with AF, clinicians use tools with various clinical, imaging and patient characteristics to weigh stroke risk against therapy-associated bleeding risk.
Aim: This article reviews published literature and summarizes available risk stratification tools for stroke and bleeding prediction in patients with AF.
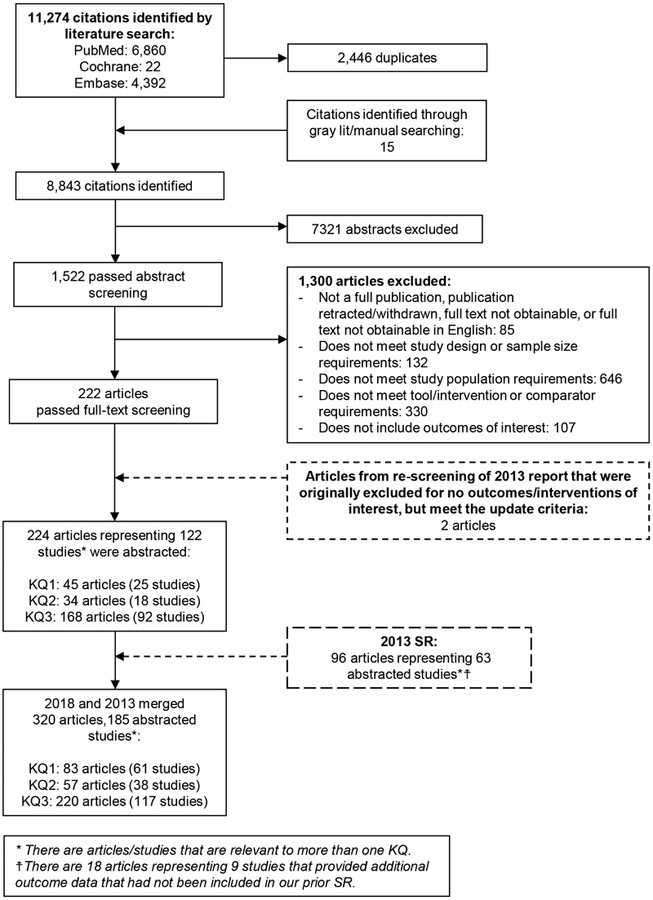
Methods: We searched for English-language studies in PubMed, Embase and the Cochrane Database of Systematic Reviews published between 1 January 2000 and 14 February 2018. Two reviewers screened citations for studies that examined tools for predicting thromboembolic and bleeding risks in patients with AF. Data regarding study design, patient characteristics, interventions, outcomes, quality, and applicability were extracted.
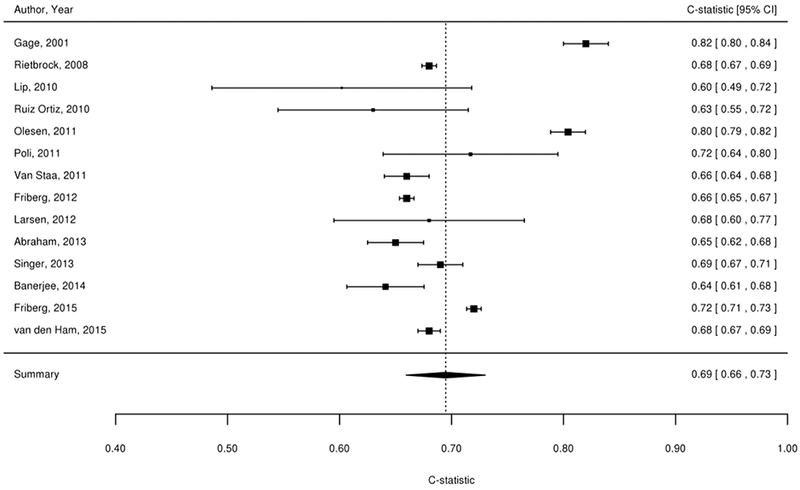
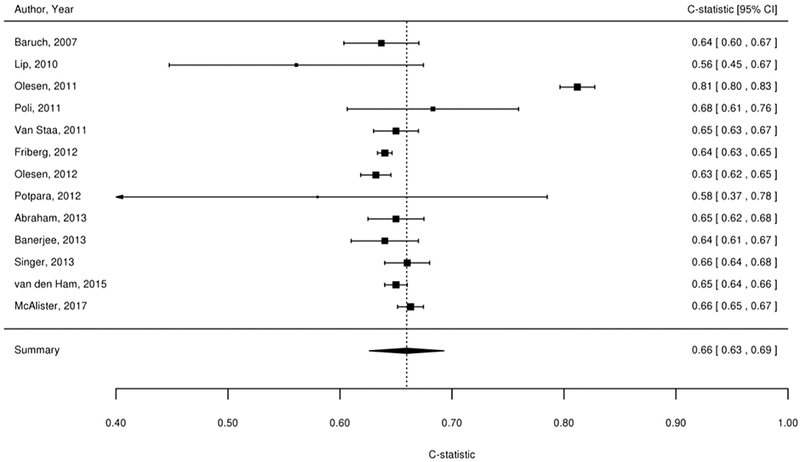
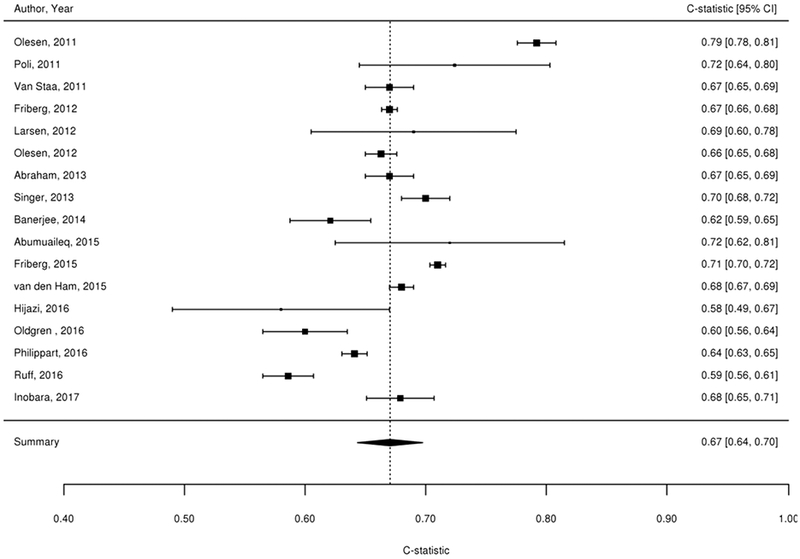
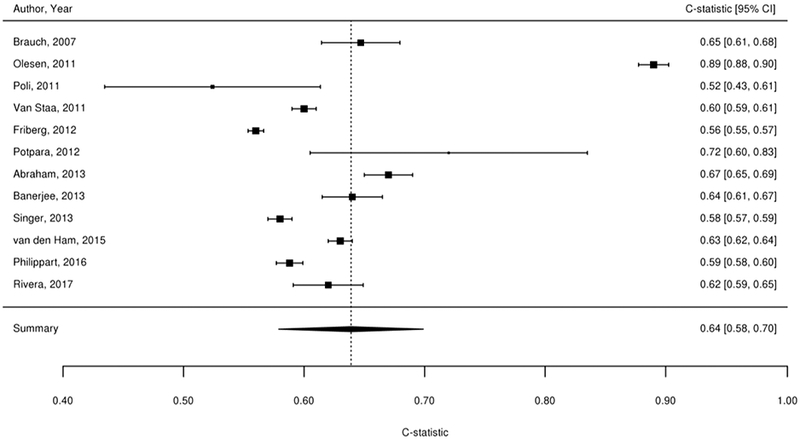
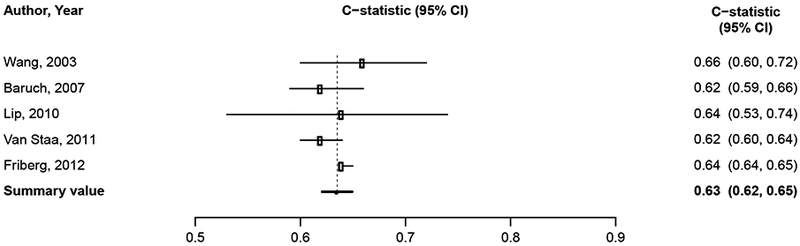
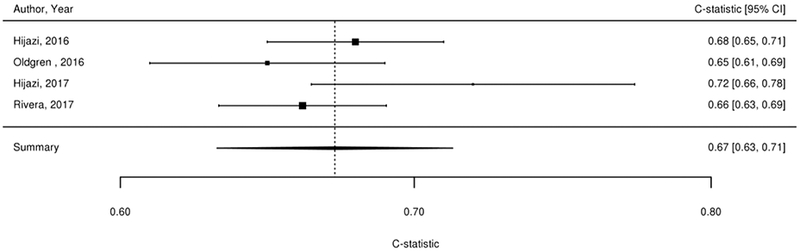
Results: Sixty-one studies were relevant to predicting thromboembolic risk and 38 to predicting bleeding risk. Data suggest that CHADS2, CHA2DS2-VASc and the age, biomarkers, and clinical history (ABC) risk scores have the best evidence for predicting thromboembolic risk (moderate strength of evidence for limited prediction ability of each score) and that HAS-BLED has the best evidence for predicting bleeding risk (moderate strength of evidence).
Limitations: Studies were heterogeneous in methodology and populations of interest, setting, interventions and outcomes analysed.
Conclusion: CHADS2, CHA2DS2-VASc and ABC scores have the best prediction for stroke events, and HAS-BLED provides the best prediction for bleeding risk. Future studies should define the role of imaging tools and biomarkers in enhancing the accuracy of risk prediction tools.
Primary funding source: Patient-Centered Outcomes Research Institute (PROSPERO #CRD42017069999).
Georg Thieme Verlag KG Stuttgart · New York.
Conflict of interest statement
None.
Figures
References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics--2015 update: a report from the American Heart Association. Circulation 2015;131(4):e29–322. - PubMed
-
- Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001;285(18):2370–2375. - PubMed
-
- Furberg CD, Psaty BM, Manolio TA, Gardin JM, Smith VE, Rautaharju PM. Prevalence of atrial fibrillation in elderly subjects (the Cardiovascular Health Study). Am J Cardiol 1994;74(3):236–241. - PubMed
-
- Lee WC, Lamas GA, Balu S, Spalding J, Wang Q, Pashos CL. Direct treatment cost of atrial fibrillation in the elderly American population: a Medicare perspective. J Med Econ 2008;11(2):281–298. - PubMed
-
- Thrall G, Lane D, Carroll D, Lip GY. Quality of life in patients with atrial fibrillation: a systematic review. Am J Med 2006;119(5):448 e441–419. - PubMed
