

Intensive therapy and remissions in rheumatoid arthritis: a systematic review
- PMID: 30376836
- PMCID: PMC6208111
- DOI: 10.1186/s12891-018-2302-5
Intensive therapy and remissions in rheumatoid arthritis: a systematic review
Abstract
Background: We systematically reviewed the effectiveness of intensive treatment strategies in achieving remission in patients with both early and established Rheumatoid Arthritis (RA).
Methods: A systematic literature review and meta-analysis evaluated trials and comparative studies reporting remission in RA patients treated intensively with disease modifying anti-rheumatic drugs (DMARDs), biologics and Janus Kinase (JAK) inhibitors. Analysis used RevMan 5.3 to report relative risks (RR) in random effects models with 95% confidence intervals (CI).
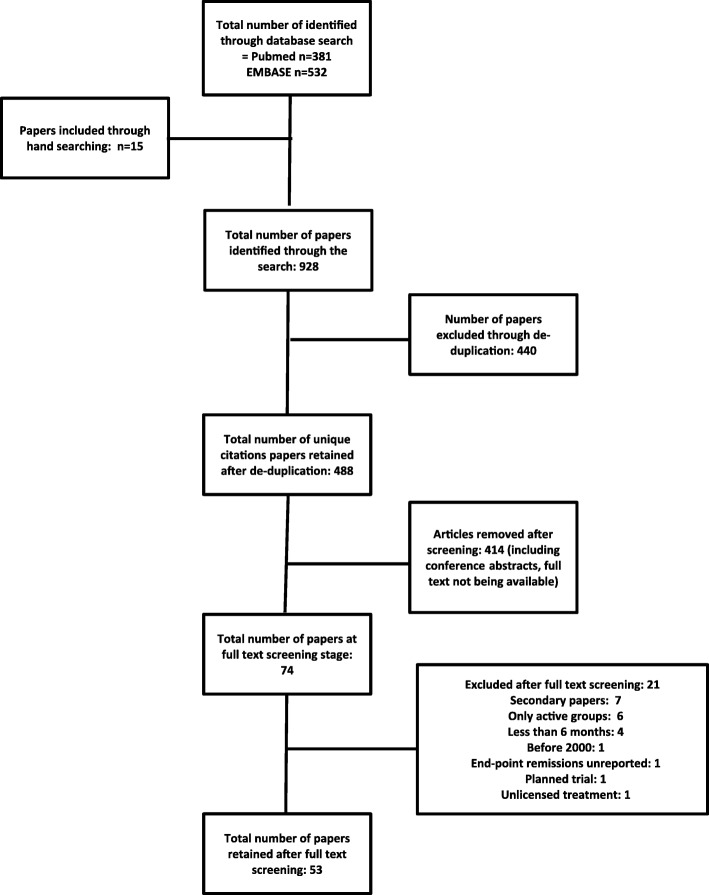
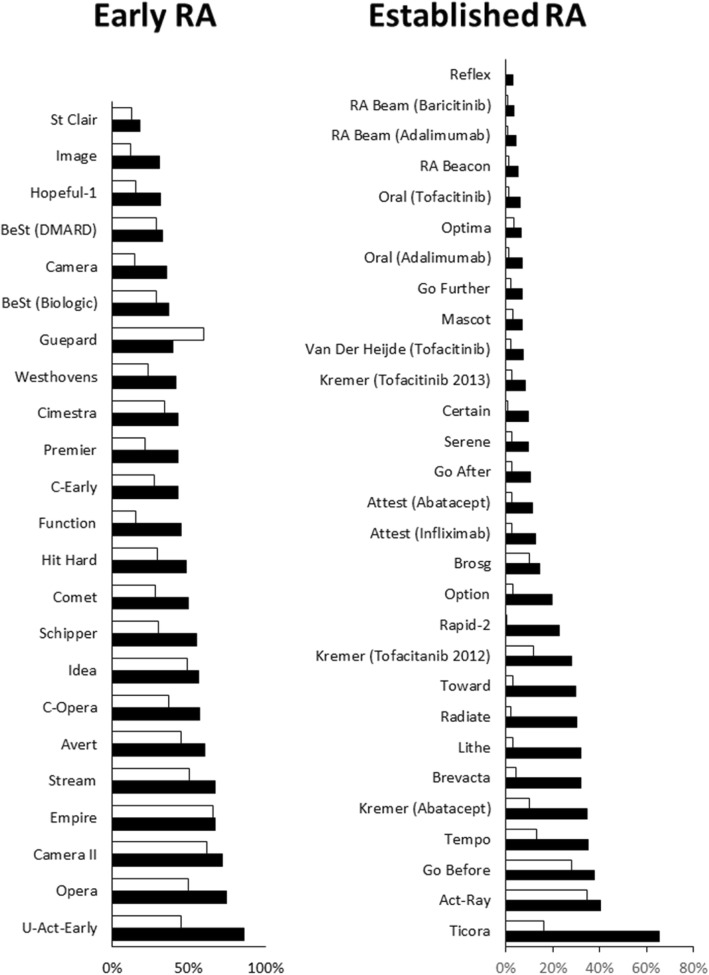
Results: We identified 928 publications: 53 studies were included (48 superiority studies; 6 head-to-head trials). In the superiority studies 3013/11259 patients achieved remission with intensive treatment compared with 1211/8493 of controls. Analysis of the 53 comparisons showed a significant benefit for intensive treatment (RR 2.23; 95% CI 1.90, 2.61). Intensive treatment increased remissions in both early RA (23 comparisons; RR 1.56; 1.38, 1.76) and established RA (29 comparisons RR 4.21, 2.92, 6.07). All intensive strategies (combination DMARDs, biologics, JAK inhibitors) increased remissions. In the 6 head-to-head trials 317/787 patients achieved remission with biologics compared with 229/671 of patients receiving combination DMARD therapies and there was no difference between treatment strategies (RR 1.06; 0.93. 1.21). There were differences in the frequency of remissions between early and established RA. In early RA the frequency of remissions with active treatment was 49% compared with 34% in controls. In established RA the frequency of remissions with active treatment was 19% compared with 6% in controls.
Conclusions: Intensive treatment with combination DMARDs, biologics or JAK inhibitors increases the frequency of remission compared to control non-intensive strategies. The benefits are seen in both early and established RA.
Keywords: Early or established rheumatoid arthritis; Outcome; Remission; Treatment response.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was not required for this systematic review, as it is not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Smolen JS, Landewe R, Bijlsma J, Burmester G, Chatzidionysiou K, Dougados M, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann Rheum Dis. 2017;76:960–977. doi: 10.1136/annrheumdis-2016-210715. - DOI - PubMed
-
- Singh JA, Saag KG, Bridges SL, Jr, Akl EA, Bannuru RR, Sullivan MC, et al. 2015 American College of Rheumatology Guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016;68:1–26. - PubMed
-
- Bykerk VP, Akhavan P, Hazlewood GS, Schieir O, Dooley A, Haraoui B, et al. Canadian rheumatology association recommendations for pharmacological management of rheumatoid arthritis with traditional and biologic disease-modifying antirheumatic drugs. J Rheumatol. 2012;39:1559–1582. doi: 10.3899/jrheum.110207. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
