

EPURE Transplant (Eplerenone in Patients Undergoing Renal Transplant) study: study protocol for a randomized controlled trial
- PMID: 30376884
- PMCID: PMC6208100
- DOI: 10.1186/s13063-018-2956-1
EPURE Transplant (Eplerenone in Patients Undergoing Renal Transplant) study: study protocol for a randomized controlled trial
Abstract
Background: Despite advances in immunosuppressive therapy, kidney graft survival has failed to improve during the last decades. Ischemia/reperfusion injury (IRI) is one of the main pathophysiological mechanisms underlying delayed graft function, which is associated with poor long-term graft survival. Due to organ shortage, the proportion of grafts from expanded criteria donors (ECDs) is ever growing. These grafts may particularly benefit from IRI prevention. In preclinical models, mineralocorticoid receptor antagonists (MRAs) have been shown to efficiently prevent IRI. This study aims to assess the effect of MRA administration in the early phase of kidney transplantation (KT) among recipients of ECD grafts on mid-term graft function.
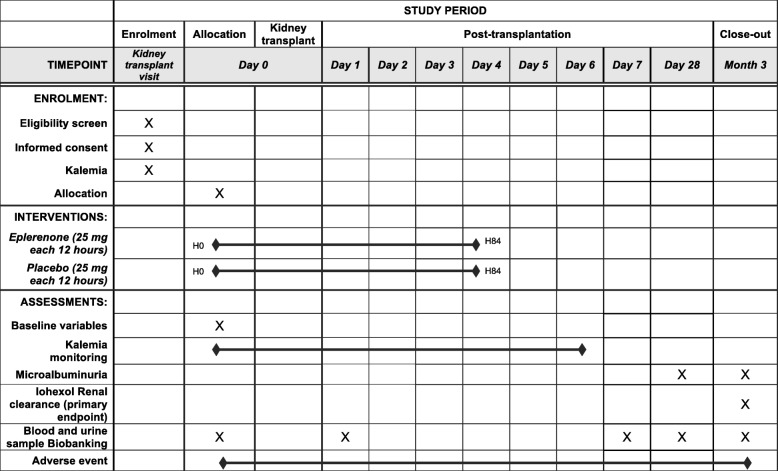
Methods/design: This is a multicenter, double-blind, placebo-controlled, randomized clinical trial. Patients on hemodialysis and undergoing a single or a dual KT from an ECD will be eligible for inclusion. We plan to randomize 132 patients. Included patients will be randomized (1:1) to receive either eplerenone 25 mg every 12 h during 4 days (the first dose being administered just prior to KT) or placebo. The primary outcome is graft function at 3 months, assessed by glomerular filtration rate (GFR, in mL/min/1.73m2) measured using iohexol clearance. Secondary outcomes include (1) proportion of patients with either dialysis dependency or a GFR < 30 mL/min/1.73m2 at 3 months, (2) proportion of patients with immediate, slow, or delayed graft function, (3) proteinuria at 3 months, (4) occurrence of hyperkalemia during the first week following KT, (5) length of hospital stay for the KT, and (6) occurrence of biopsy-proven acute rejection in the first 3 months following KT. Estimated GFR, graft, and patient survival will also be collected at 1, 3, and 10 years via the national database of organ recipients.
Discussion: Improvement of ECD grafts is a public health priority, since better ECD outcomes could eventually limit organ shortage. MRA administration in the early phase of KT may prevent IRI and subsequently improve mid-term graft function. The trial will also assess the safety of MRA administration in this population, primarily the absence of threatening hyperkalemia.
Trial registration: ClinicalTrials.gov, NCT02490904 . Registered on 1 July 2015.
Keywords: Expanded criteria donor; Ischemia/reperfusion lesions; Kidney transplantation; Mineralocorticoid receptor antagonist; Randomized controlled trial.
Conflict of interest statement
Ethics approval and consent to participate
The trial has been approved by the French regulatory agency (Agence nationale de la sécurité du medicament et des produits de santé: ANSM) and the appropriate Ethics Committee (Comité de Protection des Personnes: CPP). Written informed consent will be obtained from all participants.
Consent for publication
All authors have read and approved the final submitted version of this manuscript.
Competing interests
FJ received a research grant from BAYER. The remaining authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, Held PJ, Port FK. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341:1725–1730. doi: 10.1056/NEJM199912023412303. - DOI - PubMed
-
- Liem YS, Bosch JL, Arends LR, Heijenbrok-Kal MH, Hunink MG. Quality of life assessed with the Medical Outcomes Study Short Form 36-Item Health Survey of patients on renal replacement therapy: a systematic review and meta-analysis. Value Health. 2007;10:390–397. doi: 10.1111/j.1524-4733.2007.00193.x. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
