

Prediction of the operative time for hysteroscopic myomectomy for leiomyomas penetrating the intramural cavity using leiomyoma weight and clinical characteristics of patients
- PMID: 30377404
- PMCID: PMC6194328
- DOI: 10.1002/rmb2.12228
Prediction of the operative time for hysteroscopic myomectomy for leiomyomas penetrating the intramural cavity using leiomyoma weight and clinical characteristics of patients
Abstract
Purpose: To preoperatively predict the operative time (OT) for hysteroscopic myomectomy for G1 or G2 leiomyoma based on leiomyoma weight.
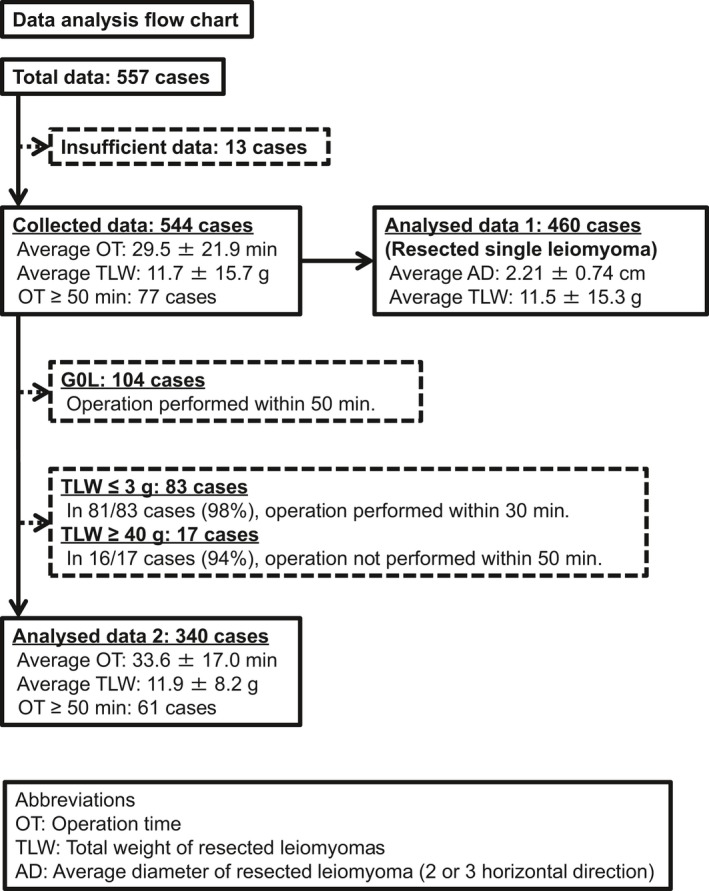
Methods: The data from 544 patients who underwent one-step hysteroscopic myomectomy were analyzed retrospectively. A total of 340 patients with leiomyoma penetrating the intramural cavity were identified as suitable candidates for calculation of the OT based on leiomyoma weight; we considered leiomyoma weight to be the most objective parameter for evaluating leiomyoma tissues. Additionally, 460 patients with a single leiomyoma were analyzed to estimate the weight of the resected leiomyoma based on its diameter.
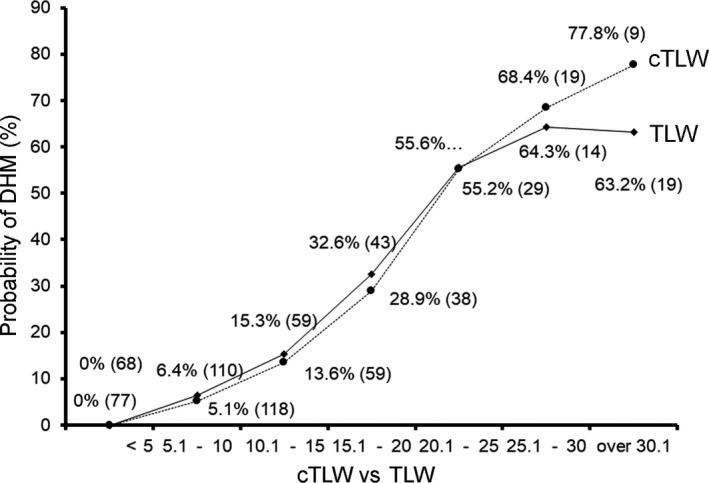
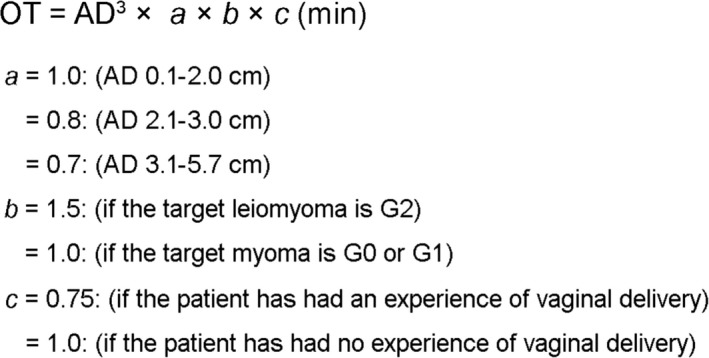
Results: Considering total leiomyoma weight (TLW) and two additional coefficients (1.5: G2 leiomyoma, 0.75: vaginal parity of the patient), we demonstrated that our formula correlated well with OT (R 2 = 0.72). TLW also correlated well with the cube of the average diameter (AD) of leiomyomas (R 2 = 0.89). Predicting TLW significantly improved the application of specific coefficients depending on its value (1.0: AD 0.1-2.0 cm, 0.8: AD 2.1-3.0 cm, 0.7: AD 3.1-5.7 cm).
Conclusion: The OT for hysteroscopic myomectomy of intracavital leiomyoma can be predicted prior to surgery using simple clinical information of the target leiomyoma and the patient.
Keywords: average diameter; degree of protrusion; operation time; patient parity; total leiomyoma weight.
Figures
Similar articles
-
A new uterine endometrium preservation hysteroscopic myomectomy: Introduction of improved procedures and a retrospective analysis of 94 cases.Eur J Obstet Gynecol Reprod Biol X. 2024 Nov 14;24:100354. doi: 10.1016/j.eurox.2024.100354. eCollection 2024 Dec. Eur J Obstet Gynecol Reprod Biol X. 2024. PMID: 39639964 Free PMC article.
-
Single-step hysteroscopic myomectomy for submucous leiomyoma.Turk J Obstet Gynecol. 2020 Jun;17(2):139-142. doi: 10.4274/tjod.galenos.2020.64280. Epub 2020 Jul 29. Turk J Obstet Gynecol. 2020. PMID: 32850190 Free PMC article.
-
Predicting success of single step hysteroscopic myomectomy: A single centre large cohort study of single myomas.Int J Surg. 2015 Oct;22:10-4. doi: 10.1016/j.ijsu.2015.07.714. Epub 2015 Aug 12. Int J Surg. 2015. PMID: 26277533
-
One-step hysteroscopic myomectomy: unusual cases and a review of the literature.J Laparoendosc Adv Surg Tech A. 2004 Dec;14(6):390-4. doi: 10.1089/lap.2004.14.390. J Laparoendosc Adv Surg Tech A. 2004. PMID: 15684788 Review.
-
Hysteroscopy for treating subfertility associated with suspected major uterine cavity abnormalities.Cochrane Database Syst Rev. 2018 Dec 5;12(12):CD009461. doi: 10.1002/14651858.CD009461.pub4. Cochrane Database Syst Rev. 2018. PMID: 30521679 Free PMC article.
Cited by
-
A new uterine endometrium preservation hysteroscopic myomectomy: Introduction of improved procedures and a retrospective analysis of 94 cases.Eur J Obstet Gynecol Reprod Biol X. 2024 Nov 14;24:100354. doi: 10.1016/j.eurox.2024.100354. eCollection 2024 Dec. Eur J Obstet Gynecol Reprod Biol X. 2024. PMID: 39639964 Free PMC article.
References
-
- Mazzon I, Bettocchi S, Fascilla F, et al. Resectoscopic myomectomy. Minerva Ginecol. 2016;68(3):334‐344. - PubMed
-
- Cravello L, Stolla V, Bretelle F, Roger V, Blanc B. Hysteroscopic resection of endometrial polyps: a study of 195 cases. Eur J Obstet Gynecol Reprod Biol. 2000;93(2):131‐134. - PubMed
-
- Darwish A. Modified hysteroscopic myomectomy of large submucous fibroids. Gynecol Obstet Invest. 2003;56(4):192‐196. - PubMed
-
- Cheng Y‐M, Lin B‐L. Modified sonohysterography immediately after hysteroscopy in the diagnosis of submucous myoma. J Am Assoc Gynecol Laparosc. 2002;9(1):24‐28. - PubMed
-
- Di Spiezio SA, Mazzon I, Bramante S, et al. Hysteroscopic myomectomy: a comprehensive review of surgical techniques. Hum Reprod Update. 2008;14(2):101‐119. - PubMed
LinkOut - more resources
Full Text Sources