

Effect of L-arginine on energy metabolism, skeletal muscle and brown adipose tissue in South Asian and Europid prediabetic men: a randomised double-blinded crossover study
- PMID: 30377712
- PMCID: PMC6290676
- DOI: 10.1007/s00125-018-4752-6
Effect of L-arginine on energy metabolism, skeletal muscle and brown adipose tissue in South Asian and Europid prediabetic men: a randomised double-blinded crossover study
Abstract
Aims/hypothesis: Individuals of South Asian origin are at increased risk of developing type 2 diabetes mellitus and associated comorbidities compared with Europids. Disturbances in energy metabolism may contribute to this increased risk. Skeletal muscle and possibly also brown adipose tissue (BAT) are involved in human energy metabolism and nitric oxide (NO) is suggested to play a pivotal role in regulating mitochondrial biogenesis in both tissues. We aimed to investigate the effects of 6 weeks of supplementation with L-arginine, a precursor of NO, on energy metabolism by BAT and skeletal muscle, as well as glucose metabolism in South Asian men compared with men of European descent.
Methods: We included ten Dutch South Asian men (age 46.5 ± 2.8 years, BMI 30.1 ± 1.1 kg/m2) and ten Dutch men of European descent, that were similar with respect to age and BMI, with prediabetes (fasting plasma glucose level 5.6-6.9 mmol/l or plasma glucose levels 2 h after an OGTT 7.8-11.1 mmol/l). Participants took either L-arginine (9 g/day) or placebo orally for 6 weeks in a randomised double-blind crossover study. Participants were eligible to participate in the study when they were aged between 40 and 55 years, had a BMI between 25 and 35 kg/m2 and did not have type 2 diabetes. Furthermore, ethnicity was defined as having four grandparents of South Asian or white European origin, respectively. Blinding of treatment was done by the pharmacy (Hankintatukku) and an independent researcher from Leiden University Medical Center randomly assigned treatments by providing a coded list. All people involved in the study as well as participants were blinded to group assignment. After each intervention, glucose tolerance was determined by OGTT and basal metabolic rate (BMR) was determined by indirect calorimetry; BAT activity was assessed by cold-induced [18F]fluorodeoxyglucose ([18F]FDG) positron emission tomography-computed tomography scanning. In addition, a fasting skeletal muscle biopsy was taken and analysed ex vivo for respiratory capacity using a multisubstrate protocol. The primary study endpoint was the effect of L-arginine on BAT volume and activity.
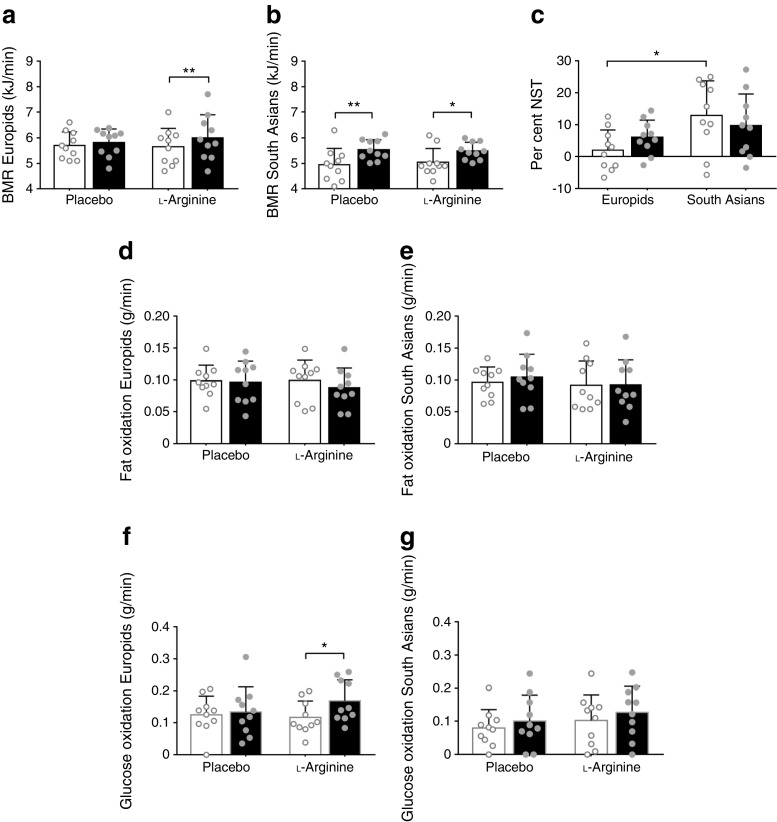
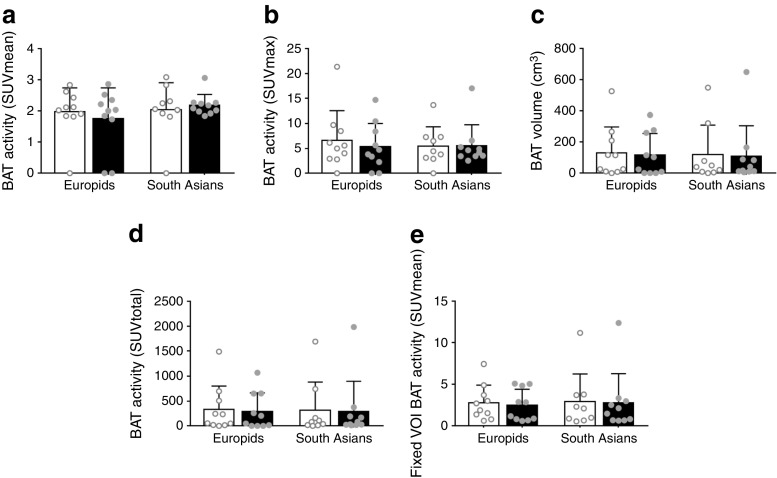
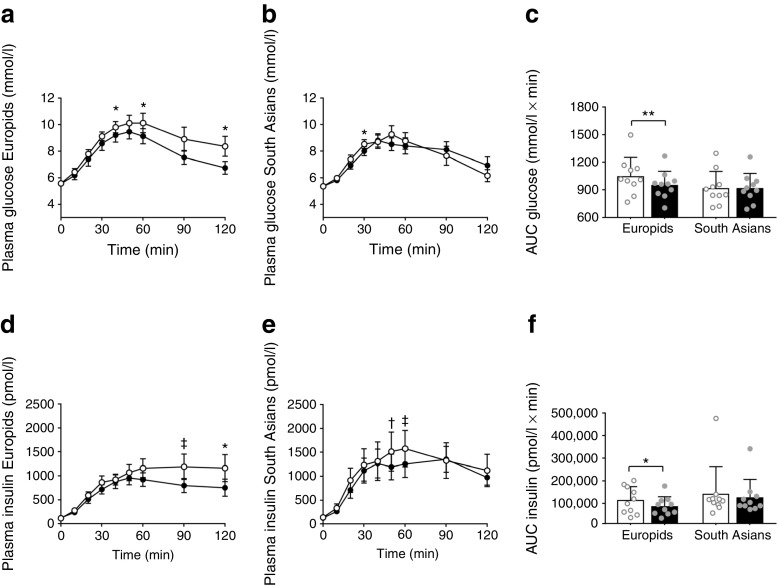
Results: L-Arginine did not affect BMR, [18F]FDG uptake by BAT or skeletal muscle respiration in either ethnicity. During OGTT, L-arginine lowered plasma glucose concentrations (AUC0-2 h - 9%, p < 0.01), insulin excursion (AUC0-2 h - 26%, p < 0.05) and peak insulin concentrations (-26%, p < 0.05) in Europid but not South Asian men. This coincided with enhanced cold-induced glucose oxidation (+44%, p < 0.05) in Europids only. Of note, in skeletal muscle biopsies several respiration states were consistently lower in South Asian men compared with Europid men.
Conclusions/interpretation: L-Arginine supplementation does not affect BMR, [18F]FDG uptake by BAT, or skeletal muscle mitochondrial respiration in Europid and South Asian overweight and prediabetic men. However, L-arginine improves glucose tolerance in Europids but not in South Asians. Furthermore, South Asian men have lower skeletal muscle oxidative capacity than men of European descent.
Funding: This study was funded by the EU FP7 project DIABAT, the Netherlands Organization for Scientific Research, the Dutch Diabetes Research Foundation and the Dutch Heart Foundation.
Trial registration: ClinicalTrials.gov NCT02291458.
Keywords: Brown adipose tissue; L-Arginine; Nitric oxide; Skeletal muscle; South Asian.
Conflict of interest statement
The authors declare that there is no duality of interest associated with this manuscript.
Figures
Similar articles
-
Effect of sitagliptin on energy metabolism and brown adipose tissue in overweight individuals with prediabetes: a randomised placebo-controlled trial.Diabetologia. 2018 Nov;61(11):2386-2397. doi: 10.1007/s00125-018-4716-x. Epub 2018 Aug 25. Diabetologia. 2018. PMID: 30145664 Free PMC article. Clinical Trial.
-
Twelve weeks of exenatide treatment increases [18F]fluorodeoxyglucose uptake by brown adipose tissue without affecting oxidative resting energy expenditure in nondiabetic males.Metabolism. 2020 May;106:154167. doi: 10.1016/j.metabol.2020.154167. Epub 2020 Jan 23. Metabolism. 2020. PMID: 31982480 Clinical Trial.
-
Brown adipose tissue volume in healthy lean south Asian adults compared with white Caucasians: a prospective, case-controlled observational study.Lancet Diabetes Endocrinol. 2014 Mar;2(3):210-7. doi: 10.1016/S2213-8587(13)70156-6. Epub 2013 Nov 12. Lancet Diabetes Endocrinol. 2014. PMID: 24622751
-
Regulation of brown adipose tissue development and white fat reduction by L-arginine.Curr Opin Clin Nutr Metab Care. 2012 Nov;15(6):529-38. doi: 10.1097/MCO.0b013e3283595cff. Curr Opin Clin Nutr Metab Care. 2012. PMID: 23075933 Review.
-
Exercise in a pill: feasibility of energy expenditure targets.Curr Drug Targets CNS Neurol Disord. 2004 Oct;3(5):389-409. doi: 10.2174/1568007043337076. Curr Drug Targets CNS Neurol Disord. 2004. PMID: 15544447 Review.
Cited by
-
Evaluation of dietary arginine supplementation to increase placental nutrient transporters in aged mares.Transl Anim Sci. 2023 Jul 5;7(1):txad058. doi: 10.1093/tas/txad058. eCollection 2023 Jan. Transl Anim Sci. 2023. PMID: 37593152 Free PMC article.
-
Impacts of Selected Dietary Nutrient Intakes on Skeletal Muscle Insulin Sensitivity and Applications to Early Prevention of Type 2 Diabetes.Adv Nutr. 2021 Jul 30;12(4):1305-1316. doi: 10.1093/advances/nmaa161. Adv Nutr. 2021. PMID: 33418570 Free PMC article. Review.
-
Dietary L-arginine supplementation increases the hepatic expression of AMP-activated protein kinase in rats.Amino Acids. 2022 Dec;54(12):1569-1584. doi: 10.1007/s00726-022-03194-w. Epub 2022 Aug 16. Amino Acids. 2022. PMID: 35972553
-
Higher Plasma Sclerostin and Lower Wnt Signaling Gene Expression in White Adipose Tissue of Prediabetic South Asian Men Compared with White Caucasian Men.Diabetes Metab J. 2020 Apr;44(2):326-335. doi: 10.4093/dmj.2019.0031. Epub 2019 Oct 31. Diabetes Metab J. 2020. PMID: 31701693 Free PMC article. Clinical Trial.
-
Short-Term Cooling Increases Plasma ANGPTL3 and ANGPTL8 in Young Healthy Lean Men but Not in Middle-Aged Men with Overweight and Prediabetes.J Clin Med. 2019 Aug 14;8(8):1214. doi: 10.3390/jcm8081214. J Clin Med. 2019. PMID: 31416197 Free PMC article.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
