

The functional consequences of sodium channel NaV 1.8 in human left ventricular hypertrophy
- PMID: 30378291
- PMCID: PMC6352890
- DOI: 10.1002/ehf2.12378
The functional consequences of sodium channel NaV 1.8 in human left ventricular hypertrophy
Abstract
Aims: In hypertrophy and heart failure, the proarrhythmic persistent Na+ current (INaL ) is enhanced. We aimed to investigate the electrophysiological role of neuronal sodium channel NaV 1.8 in human hypertrophied myocardium.
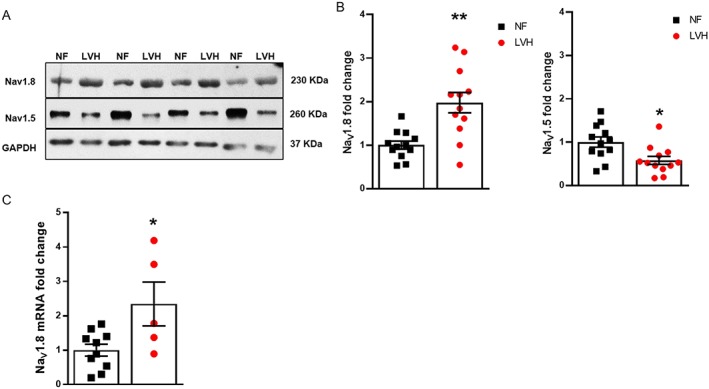
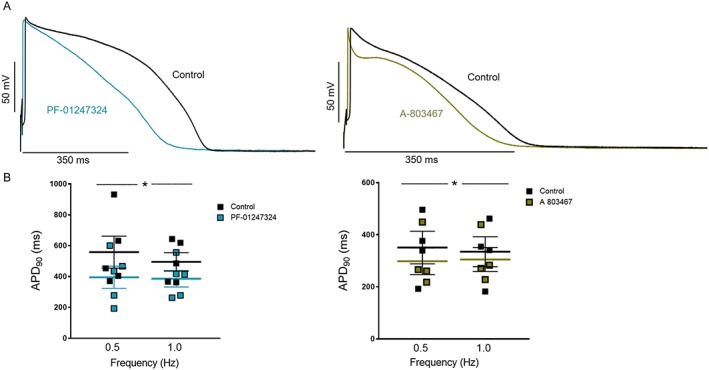
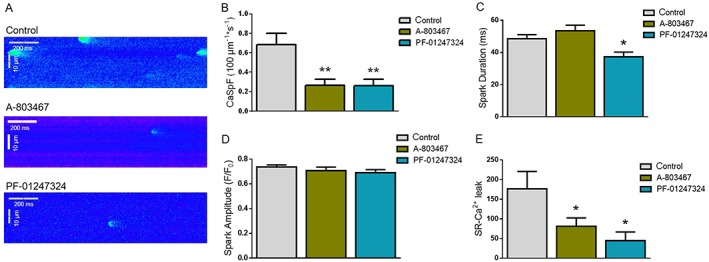
Methods and results: Myocardial tissue of 24 patients suffering from symptomatic severe aortic stenosis and concomitant significant afterload-induced hypertrophy with preserved ejection fraction was used and compared with 12 healthy controls. We performed quantitative real-time PCR and western blot and detected a significant up-regulation of NaV 1.8 mRNA (2.34-fold) and protein expression (1.96-fold) in human hypertrophied myocardium compared with healthy hearts. Interestingly, NaV 1.5 protein expression was significantly reduced in parallel (0.60-fold). Using whole-cell patch-clamp technique, we found that the prominent INaL was significantly reduced after addition of novel NaV 1.8-specific blockers either A-803467 (30 nM) or PF-01247324 (1 μM) in human hypertrophic cardiomyocytes. This clearly demonstrates the relevant contribution of NaV 1.8 to this proarrhythmic current. We observed a significant action potential duration shortening and performed confocal microscopy, demonstrating a 50% decrease in proarrhythmic diastolic sarcoplasmic reticulum (SR)-Ca2+ leak and SR-Ca2+ spark frequency after exposure to both NaV 1.8 inhibitors.
Conclusions: We show for the first time that the neuronal sodium channel NaV 1.8 is up-regulated on mRNA and protein level in the human hypertrophied myocardium. Furthermore, inhibition of NaV 1.8 reduced augmented INaL , abbreviated the action potential duration, and decreased the SR-Ca2+ leak. The findings of our study suggest that NaV 1.8 could be a promising antiarrhythmic therapeutic target and merits further investigation.
Keywords: Arrhythmias; Calcium; HFpEF; Late sodium current; Left ventricular hypertrophy; SR-Ca2+ leak; Sodium channels.
© 2018 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Figures

Similar articles
-
Contribution of the neuronal sodium channel NaV1.8 to sodium- and calcium-dependent cellular proarrhythmia.J Mol Cell Cardiol. 2020 Jul;144:35-46. doi: 10.1016/j.yjmcc.2020.05.002. Epub 2020 May 11. J Mol Cell Cardiol. 2020. PMID: 32418916
-
Contribution of sodium channel neuronal isoform Nav1.1 to late sodium current in ventricular myocytes from failing hearts.J Physiol. 2015 Mar 15;593(6):1409-27. doi: 10.1113/jphysiol.2014.278259. Epub 2014 Nov 17. J Physiol. 2015. PMID: 25772296 Free PMC article.
-
Differential regulation of sodium channels as a novel proarrhythmic mechanism in the human failing heart.Cardiovasc Res. 2018 Nov 1;114(13):1728-1737. doi: 10.1093/cvr/cvy152. Cardiovasc Res. 2018. PMID: 29931291
-
Neuronal sodium channels: emerging components of the nano-machinery of cardiac calcium cycling.J Physiol. 2017 Jun 15;595(12):3823-3834. doi: 10.1113/JP273058. Epub 2017 Mar 26. J Physiol. 2017. PMID: 28195313 Free PMC article. Review.
-
Phosphorylation of cardiac voltage-gated sodium channel: Potential players with multiple dimensions.Acta Physiol (Oxf). 2019 Mar;225(3):e13210. doi: 10.1111/apha.13210. Epub 2018 Dec 16. Acta Physiol (Oxf). 2019. PMID: 30362642 Free PMC article. Review.
Cited by
-
Pathophysiological insights into HFpEF from studies of human cardiac tissue.Nat Rev Cardiol. 2025 Feb;22(2):90-104. doi: 10.1038/s41569-024-01067-1. Epub 2024 Aug 28. Nat Rev Cardiol. 2025. PMID: 39198624 Free PMC article. Review.
-
Absence of Functional Nav1.8 Channels in Non-diseased Atrial and Ventricular Cardiomyocytes.Cardiovasc Drugs Ther. 2019 Dec;33(6):649-660. doi: 10.1007/s10557-019-06925-6. Cardiovasc Drugs Ther. 2019. PMID: 31916131 Free PMC article.
-
Patient-specific induced pluripotent stem cell properties implicate Ca2+-homeostasis in clinical arrhythmia associated with combined heterozygous RYR2 and SCN10A variants.Philos Trans R Soc Lond B Biol Sci. 2023 Jun 19;378(1879):20220175. doi: 10.1098/rstb.2022.0175. Epub 2023 May 1. Philos Trans R Soc Lond B Biol Sci. 2023. PMID: 37122207 Free PMC article.
-
Characterization of novel arrhythmogenic patterns arising secondary to heterogeneous expression and activation of Nav1.8.Front Cardiovasc Med. 2025 Mar 20;12:1546803. doi: 10.3389/fcvm.2025.1546803. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40182425 Free PMC article.
-
Mexiletine-like cellular electrophysiological effects of GS967 in canine ventricular myocardium.Sci Rep. 2021 May 5;11(1):9565. doi: 10.1038/s41598-021-88903-3. Sci Rep. 2021. PMID: 33953276 Free PMC article.
References
-
- Savage DD, Garrison RJ, Kannel WB, Levy D, Anderson SJ, Stokes J III, Feinleib M, Castelli WP. The spectrum of left ventricular hypertrophy in a general population sample: the Framingham Study. Circulation 1987; 75: I26–I33. - PubMed
-
- Kannel WB. Prevalence and natural history of electrocardiographic left ventricular hypertrophy. Am J Med 1983; 75: 4–11. - PubMed
-
- Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med 1990; 322: 1561–1566. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, Gonzalez‐Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Rev Esp Cardiol (Engl Ed) 2016; 69: 1167. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
