

Development and validation of a new method for indirect estimation of neonatal, infant, and child mortality trends using summary birth histories
- PMID: 30379812
- PMCID: PMC6209133
- DOI: 10.1371/journal.pmed.1002687
Development and validation of a new method for indirect estimation of neonatal, infant, and child mortality trends using summary birth histories
Abstract
Background: The addition of neonatal (NN) mortality targets in the Sustainable Development Goals highlights the increased need for age-specific quantification of mortality trends, detail that is not provided by summary birth histories (SBHs). Several methods exist to indirectly estimate trends in under-5 mortality from SBHs; however, efforts to monitor mortality trends in important age groups such as the first month and first year of life have yet to utilize the vast amount of SBH data available from household surveys and censuses.
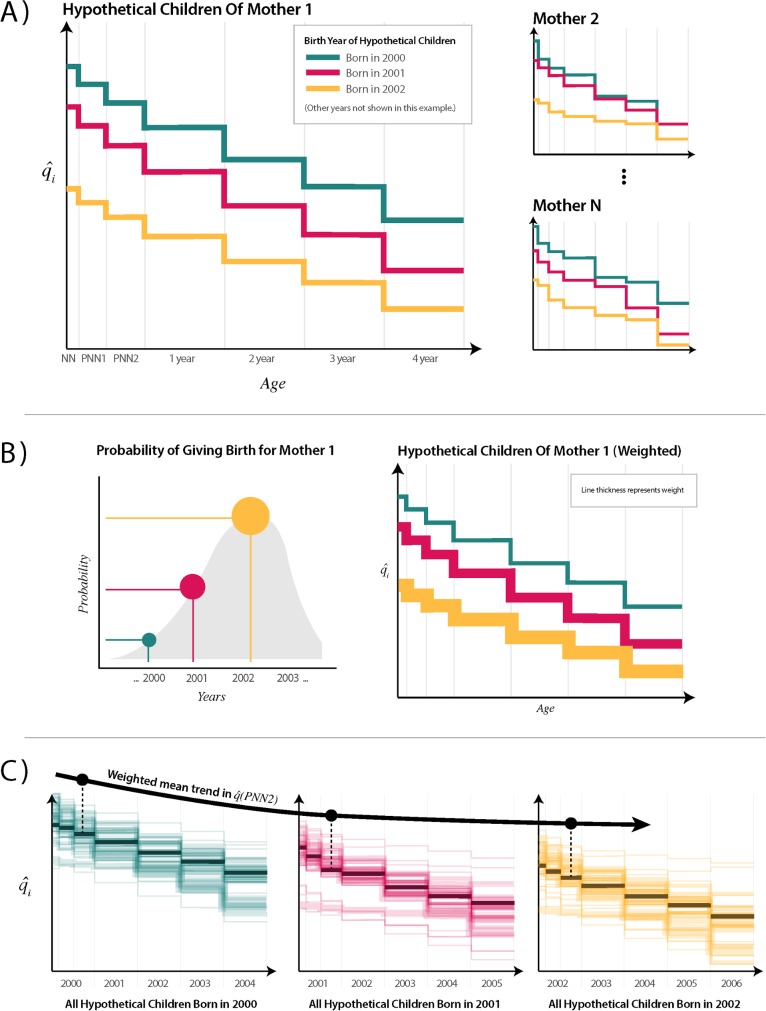
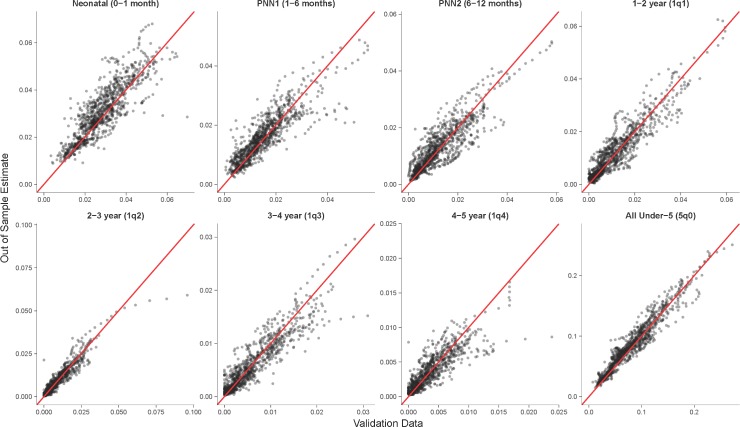
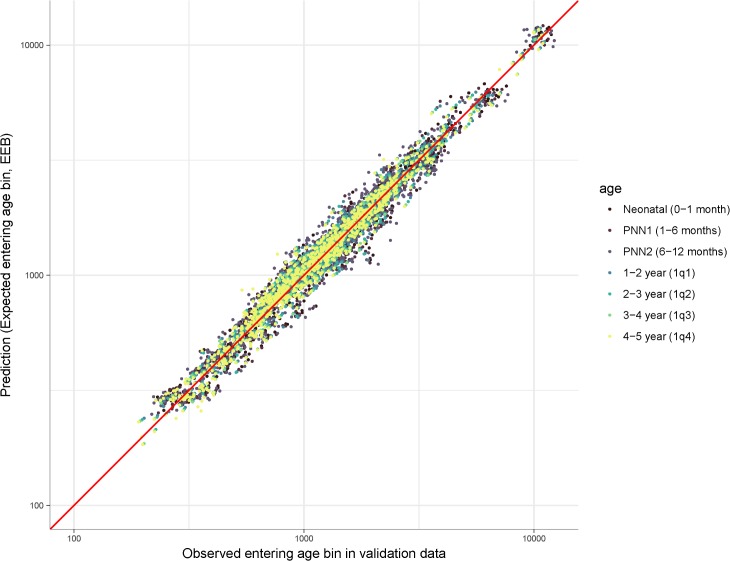
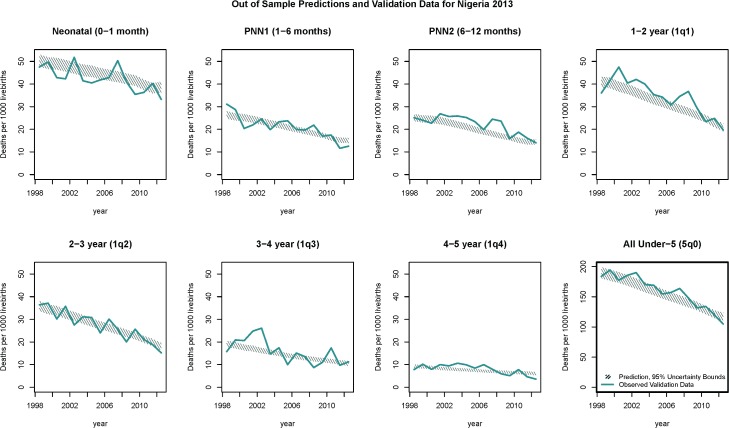
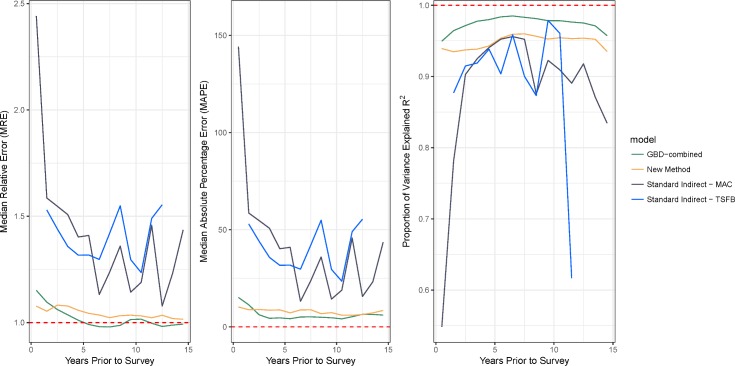
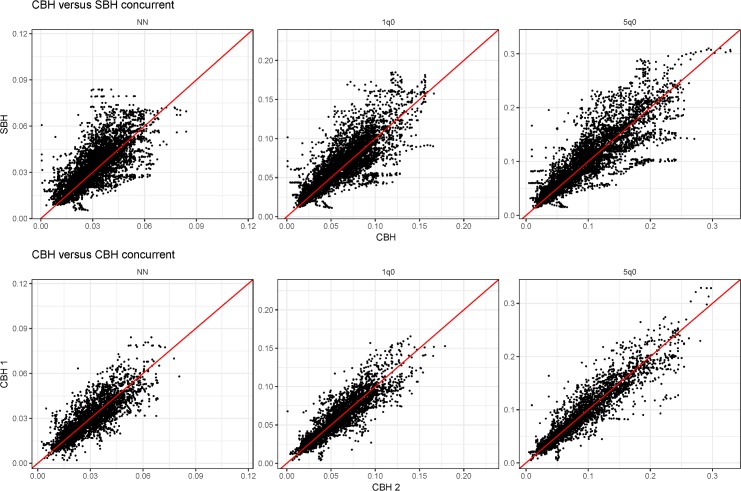
Methods and findings: We analyzed 243 Demographic and Health Surveys (DHS) from 76 countries, which collected both complete and SBHs from 8.5 million children from 2.3 million mothers to develop a new empirically based method to indirectly estimate time trends in age-specific mortality. We used complete birth history (CBH) data to train a discrete hazards generalized additive model in order to predict individual hazard functions for children based on individual-, mother-, and country-year-level covariates. Individual-level predictions were aggregated over time by assigning probability weights to potential birth years from mothers from SBH data. Age-specific estimates were evaluated in three ways: using cross-validation, using an external database of an additional 243 non-DHS census and survey data sources, and comparing overall under-5 mortality to existing indirect methods. Our model was able to closely approximate trends in age-specific child mortality. Depending on age, the model was able to explain between 80% and 95% of the variation in the validation data. Bias was close to zero in every age, with median relative errors spanning from 0.96 to 1.09. For trends in all under-5s, performance was comparable to the methods used for the Global Burden of Disease (GBD) study and significantly better than the standard indirect (Brass) method, especially in the 5 years preceding a survey. For the 15 years preceding surveys, the new method and GBD methods could explain more than 95% of the variation in the validation data for under-5s, whereas the standard indirect variants tested could only explain up to 88%. External validation using census and survey data found close agreement with concurrent direct estimates of mortality in the NN and infant age groups. As a predictive method based on empirical data, one limitation is that potential issues in these training data could be reflected in the resulting application of the method out of sample.
Conclusions: This new method for estimating child mortality produces results that are comparable to current best methods for indirect estimation of under-5 mortality while additionally producing age-specific estimates. Use of such methods allows researchers to utilize a massive amount of SBH data for estimation of trends in NN and infant mortality. Systematic application of these methods could further improve the evidence base for monitoring of trends and inequalities in age-specific child mortality.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- You D, Hug L, Ejdemyr S, Idele P, Hogan D, Mathers C, et al. Global, regional, and national levels and trends in under-5 mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. The Lancet. 2015;386: 2275–2286. 10.1016/S0140-6736(15)00120-8 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
