

Potential role of CSF cytokine profiles in discriminating infectious from non-infectious CNS disorders
- PMID: 30379898
- PMCID: PMC6209186
- DOI: 10.1371/journal.pone.0205501
Potential role of CSF cytokine profiles in discriminating infectious from non-infectious CNS disorders
Abstract
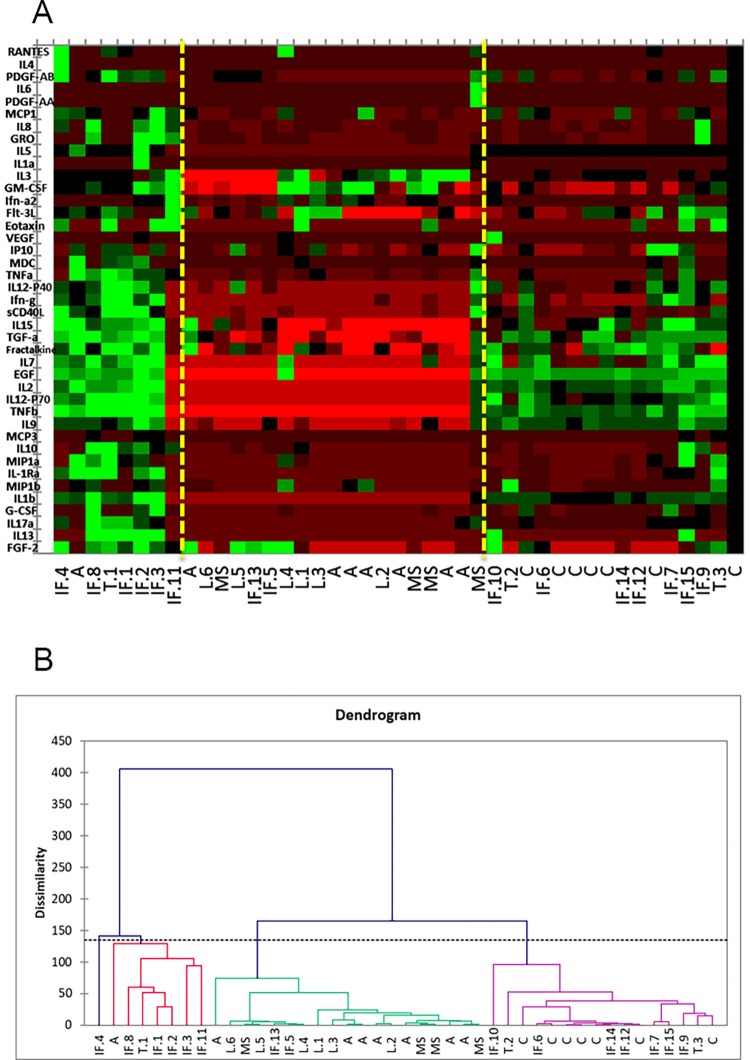
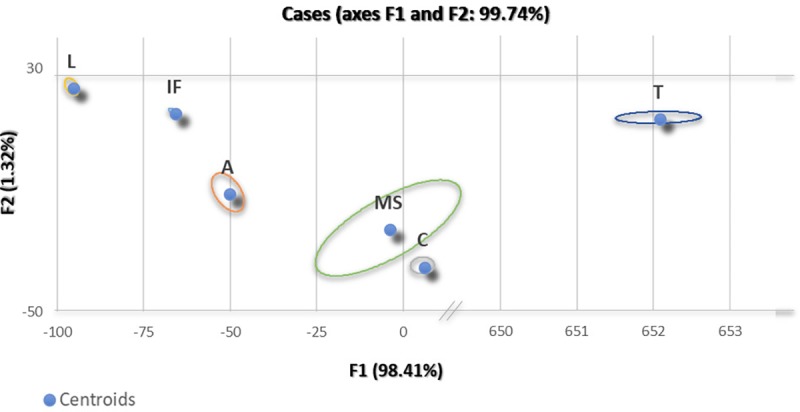
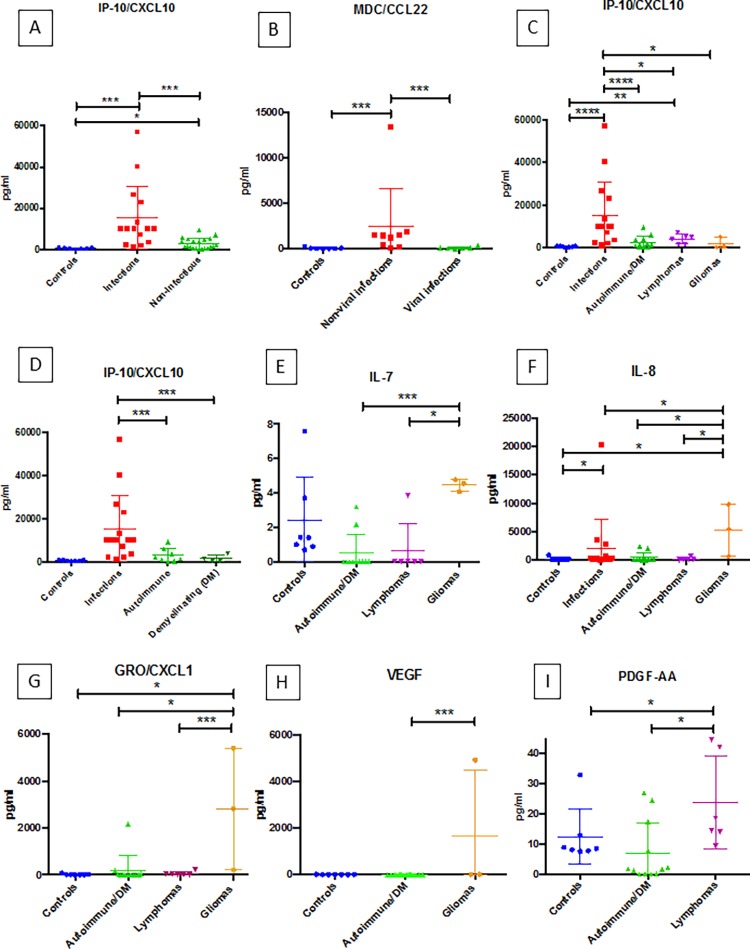
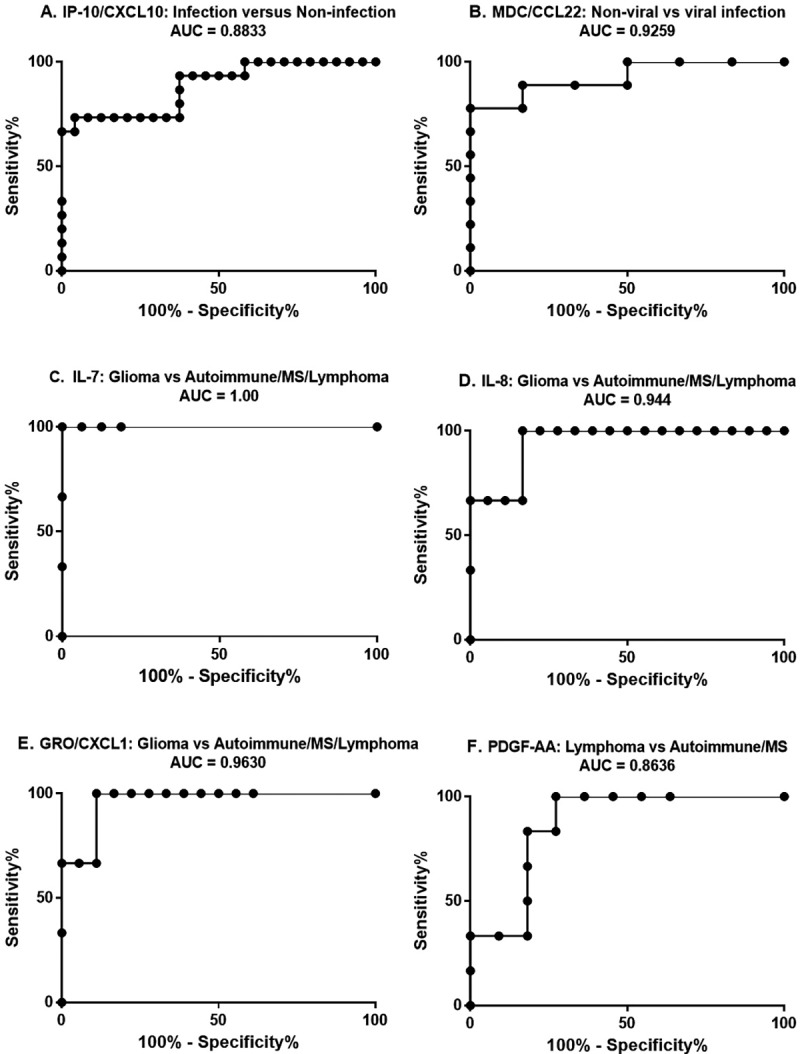
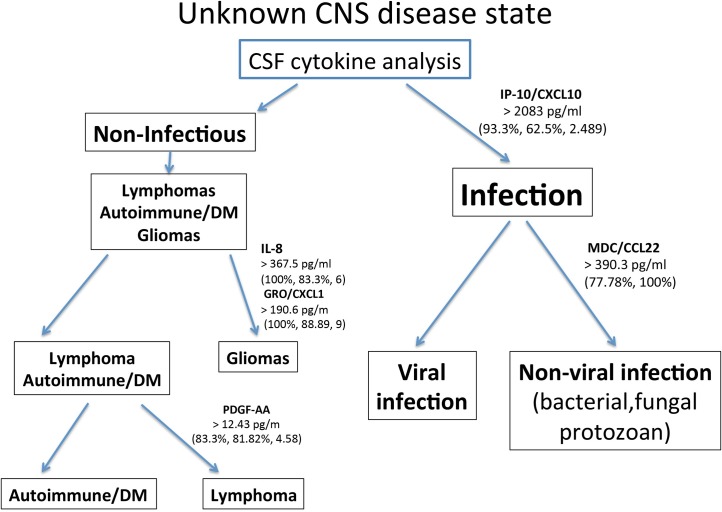
Current laboratory testing of cerebrospinal fluid (CSF) does not consistently discriminate between different central nervous system (CNS) disease states. Rapidly distinguishing CNS infections from other brain and spinal cord disorders that share a similar clinical presentation is critical. New approaches focusing on aspects of disease biology, such as immune response profiles that can have stimulus-specific attributes, may be helpful. We undertook this preliminary proof-of-concept study using multiplex ELISA to measure CSF cytokine levels in various CNS disorders (infections, autoimmune/demyelinating diseases, lymphomas, and gliomas) to determine the potential utility of cytokine patterns in differentiating CNS infections from other CNS diseases. Both agglomerative hierarchical clustering and mixture discriminant analyses revealed grouping of CNS disease types based on cytokine expression. To further investigate the ability of CSF cytokine levels to distinguish various CNS disease states, non-parametric statistical analysis was performed. Mann-Whitney test analysis demonstrated that CNS infections are characterized by significantly higher CSF lP-10/CXCL10 levels than the pooled non-infectious CNS disorders (p = 0.0001). Within the infection group, elevated levels of MDC/CCL22 distinguished non-viral from viral infections (p = 0.0048). Each disease group of the non-infectious CNS disorders independently showed IP-10/CXCL10 levels that are significantly lower than the infection group [(autoimmune /demyelinating disorders (p = 0.0005), lymphomas (p = 0.0487), gliomas (p = 0.0294), and controls (p = 0.0001)]. Additionally, of the non-infectious diseases, gliomas can be distinguished from lymphomas by higher levels of GRO/CXCL1 (p = 0.0476), IL-7 (p = 0.0119), and IL-8 (p = 0.0460). Gliomas can also be distinguished from autoimmune/demyelinating disorders by higher levels of GRO/CXCL1 (p = 0.0044), IL-7 (p = 0.0035) and IL-8 (p = 0.0176). Elevated CSF levels of PDGF-AA distinguish lymphomas from autoimmune/demyelinating cases (p = 0.0130). Interrogation of the above comparisons using receiver operator characteristic analysis demonstrated area under the curve (AUC) values (ranging from 0.8636-1.0) that signify good to excellent utility as potential diagnostic discriminators. In conclusion, our work indicates that upon formal validation, measurement of CSF cytokine levels may have clinical utility in both identifying a CNS disorder as infectious in etiology and, furthermore, in distinguishing viral from non-viral CNS infections.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
