

The epidemiology of chronic kidney disease and the association with non-communicable and communicable disorders in a population of sub-Saharan Africa
- PMID: 30379902
- PMCID: PMC6209178
- DOI: 10.1371/journal.pone.0205326
The epidemiology of chronic kidney disease and the association with non-communicable and communicable disorders in a population of sub-Saharan Africa
Abstract
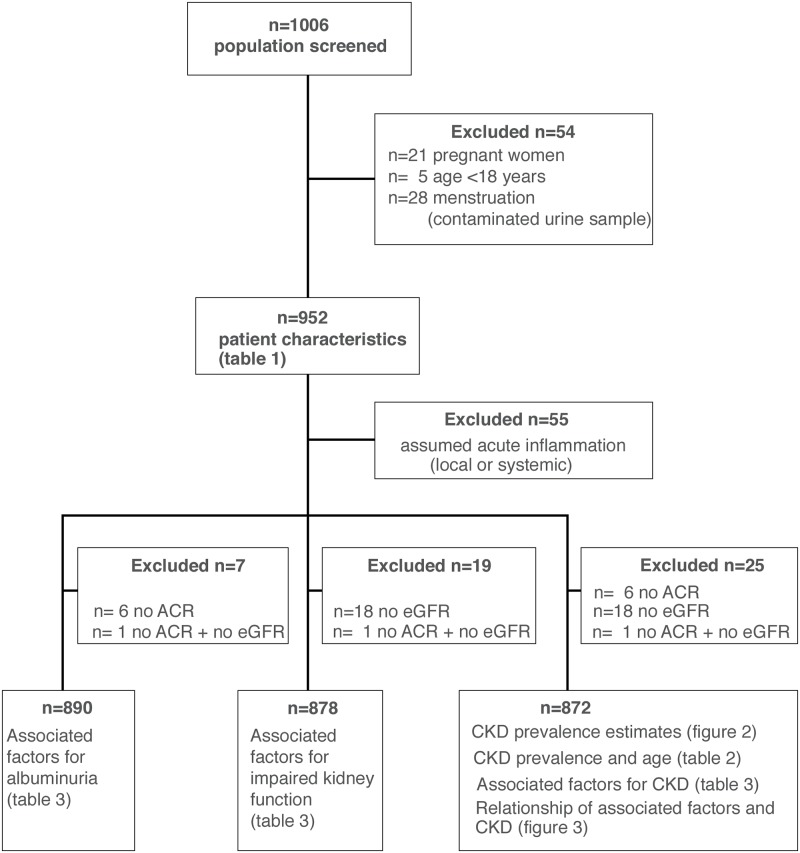
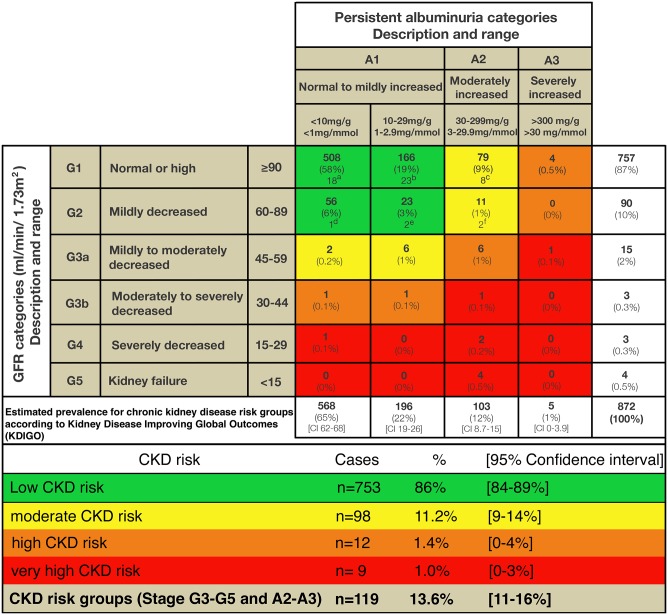
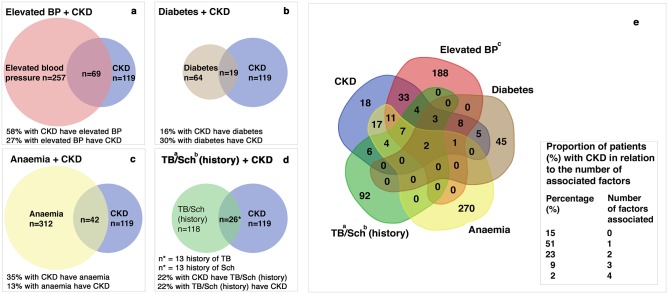
In sub-Saharan Africa (SSA), epidemiological data for chronic kidney disease (CKD) are scarce. We conducted a prospective cross-sectional study including 952 patients in an outpatient clinic in Tanzania to explore CKD prevalence estimates and the association with cardiovascular and infectious disorders. According to KDIGO, we measured albumin-to-creatinine ratio and calculated eGFR using CKD-EPI formula. Factors associated with CKD were calculated by logistic regression. Venn diagrams were modelled to visualize interaction between associated factors and CKD. Overall, the estimated CKD prevalence was 13.6% (95% CI 11-16%). Ninety-eight patients (11.2%) (95% CI 9-14%) were categorized as moderate, 12 (1.4%) (95% CI 0-4%) as high, and 9 (1%) (95% CI 0-3%) as very high risk according to KDIGO. History of tuberculosis (OR 3.75, 95% CI 1.66-8.18; p = 0.001) and schistosomiasis (OR 2.49, 95% CI 1.13-5.18; p = 0.02) were associated with CKD. A trend was seen for increasing systolic blood pressure (OR 1.02 per 1 mmHg, 95% CI 1.00-1.03; p = 0.01). Increasing BMI (OR 0.92 per 1kg/m2, 95% CI 0.88-0.96; p = <0.001) and haemoglobin (OR 0.82 per 1g/dL, 95% CI 0.72-0.94; p = 0.004) were associated with risk reduction. Diabetes was associated with albuminuria (OR 2.81, 95% CI 1.26-6.00; p = 0.009). In 85% of all CKD cases at least one of the four most common factors (hypertension, diabetes, anaemia, and history of tuberculosis or schistosomiasis) was associated with CKD. A singular associated factor was found in 61%, two in 14%, and ≥3 in 10% of all CKD cases. We observed a high prevalence estimate for CKD and found that both classical cardiovascular and neglected infectious diseases might be associated with CKD in a semi-rural population of SSA. Our finding provides further evidence for the hypothesis that the "double burden" of non-communicable and endemic infectious diseases might affect kidney health in SSA.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Levey AS, Atkins R, Coresh J, Cohen EP, Collins AJ, Eckardt KU, et al. Chronic kidney disease as a global public health problem: approaches and initiatives—a position statement from Kidney Disease Improving Global Outcomes. Kidney international. 2007;72(3):247–59. Epub 2007/06/15. 10.1038/sj.ki.5002343 . - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
