

Autoantibody-Mediated Encephalitis
- PMID: 30381132
- PMCID: PMC6234470
- DOI: 10.3238/arztebl.2018.0666
Autoantibody-Mediated Encephalitis
Abstract
Background: Acute and subacute disturbances of wakefulness and cognitive function are common neurological manifestations in the hospital and in outpatient care. An important element of the differential diagnosis was described only a few years ago: autoimmune encephalitis, a condition whose diagnosis and treatment pose an interdisciplinary challenge.
Methods: This review is based on pertinent publications from the years 2005-2017 that were retrieved by a selective search in PubMed, and on the authors' personal experience and case reports.
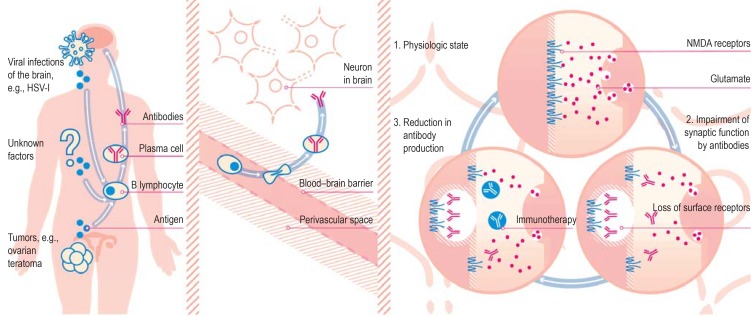
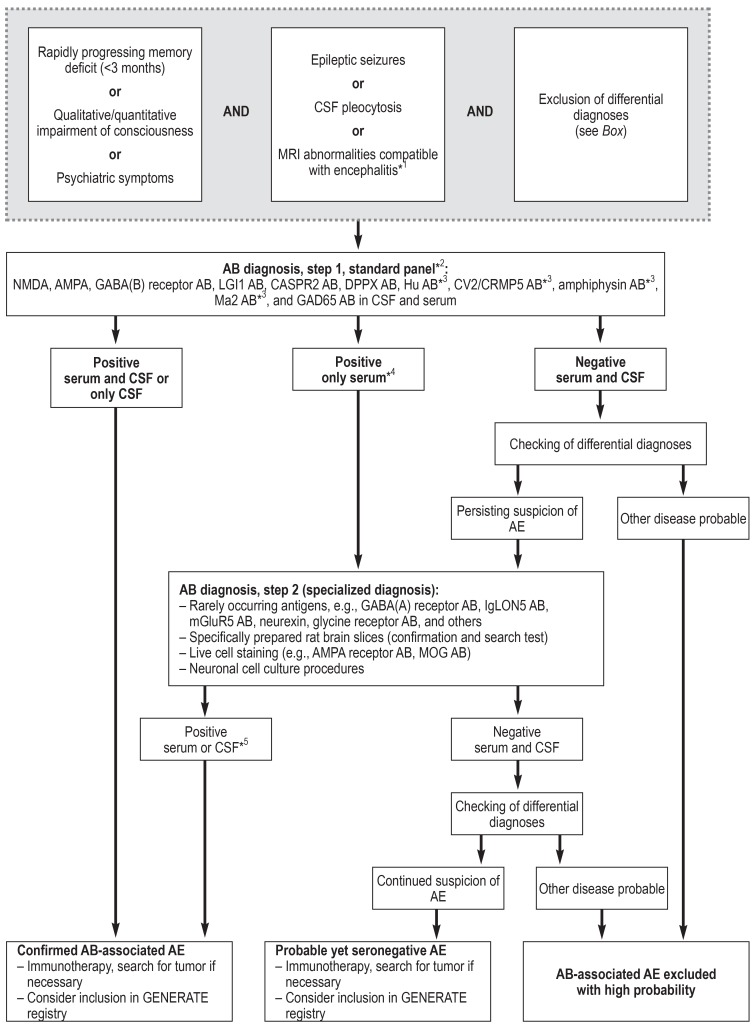
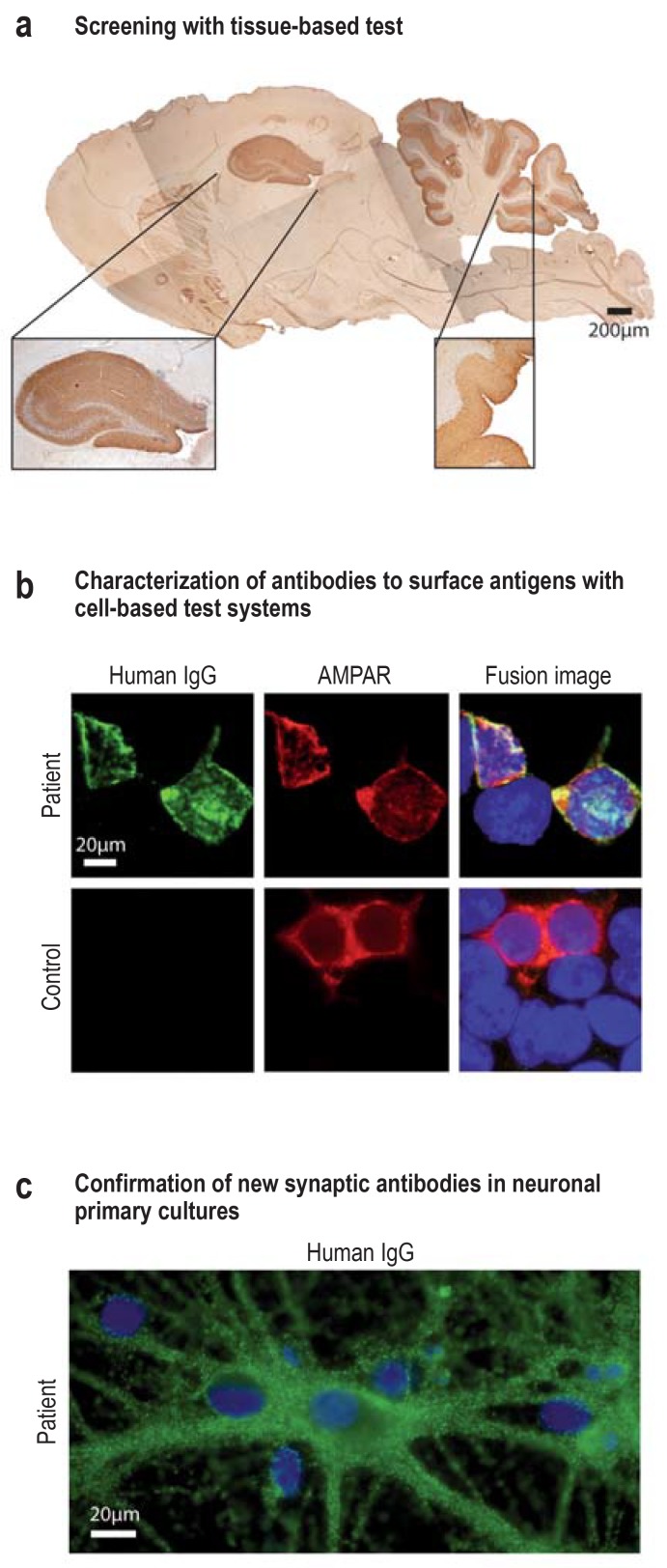
Results: The incidence of autoimmune encephalitis in Germany is estimated at 8-15 cases per million persons per year. In some patients with psychotic manifestations or impaired consciousness of acute or subacute onset, an autoimmune patho - genesis can be demonstrated by the laboratory detection of autoantibodies against neuronal target antigens (e.g., glutamate receptors). Testing of this type should be performed in patients with inflammatory changes in the cerebrospinal fluid or on magnetic resonance imaging (MRI), or those who have had an otherwise unexplained first epileptic seizure or status epilepticus. The cumulative sensitivity of testing for all potentially causative antineuronal antibodies in patients with clinically defined autoimmune encephalitis is estimated at 60-80 %. Figures on cumulative specificity are currently unavailable.
Conclusion: The detection of antineuronal antibodies in patients with the corresponding appropriate symptoms implies the diagnosis of autoimmune encephalitis. Observational studies have shown that rapidly initiated immunosuppressive treatment improves these patients' outcomes. Further studies are needed to determine the positive predictive value of antineuronal antibody detection and to develop further treatment options under randomized and controlled conditions.
Figures
References
-
- Royl G, Ploner CJ, Möckel M, Leithner C. [Neurological chief complaints in an emergency room] Nervenarzt. 2010;81:1226–1230. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical