

Maternal-fetal transmission and adverse perinatal outcomes in pregnant women infected with Zika virus: prospective cohort study in French Guiana
- PMID: 30381296
- PMCID: PMC6207920
- DOI: 10.1136/bmj.k4431
Maternal-fetal transmission and adverse perinatal outcomes in pregnant women infected with Zika virus: prospective cohort study in French Guiana
Abstract
Objectives: To estimate the rates of maternal-fetal transmission of Zika virus, adverse fetal/neonatal outcomes, and subsequent rates of asymptomatic/symptomatic congenital Zika virus infections up to the first week of life.
Design: Cohort study with prospective data collection and subsequent review of fetal/neonatal outcomes.
Settings: Referral centre for prenatal diagnosis of the French Guiana Western Hospital.
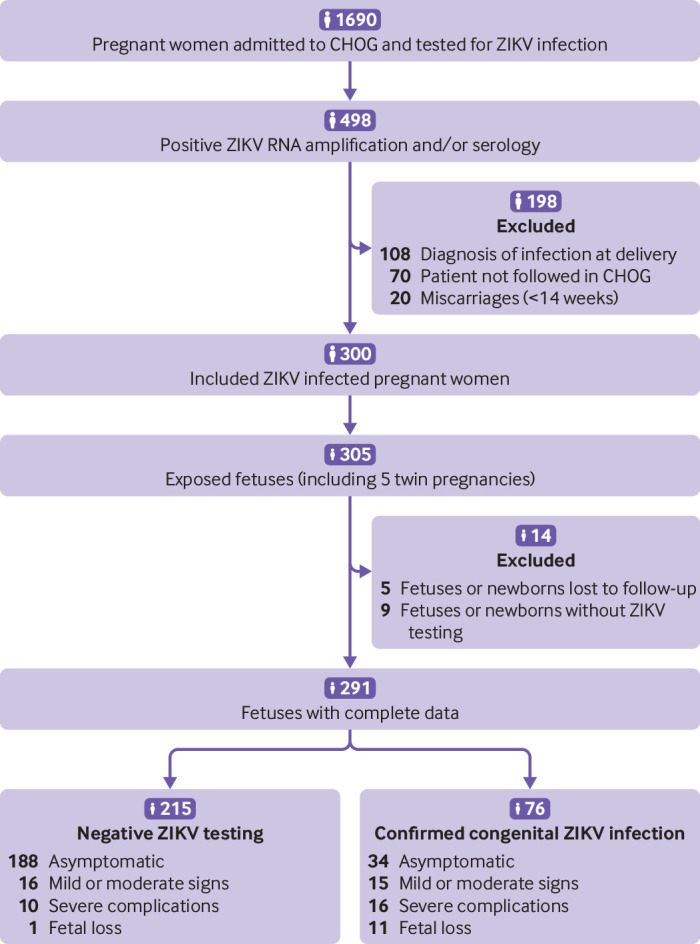
Participants: Pregnant women at any stage of pregnancy with a laboratory confirmed symptomatic or asymptomatic Zika virus infection during the epidemic period in western French Guiana. The cohort enrolled 300 participants and prospectively followed their 305 fetuses/newborns.
Main outcome measures: Rate of maternal-fetal transmission of Zika virus (amniotic fluid, fetal and neonatal blood, urine, cerebrospinal fluid, and placentas); clinical, biological, and radiological outcomes (blindly reviewed); and adverse outcomes defined as moderate signs potentially related to congenital Zika syndrome (CZS), severe complications compatible with CZS, or fetal loss. Associations between a laboratory confirmed congenital Zika virus infection and adverse fetal/neonatal outcomes were evaluated.
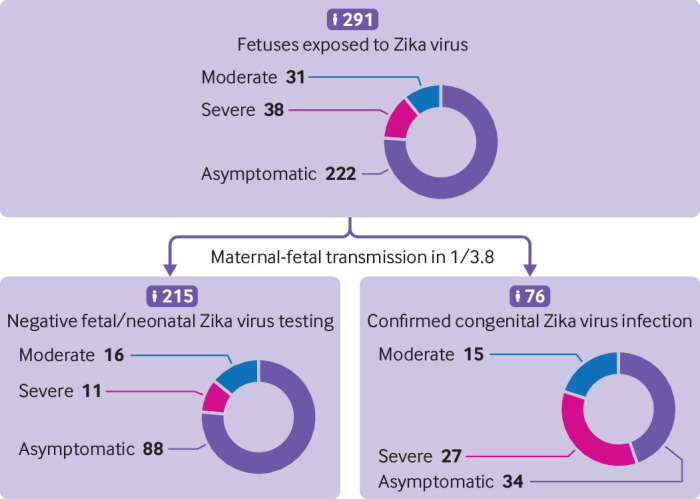
Results: Maternal-fetal transmission was documented in 26% (76/291) of fetuses/newborns with complete data. Among the Zika virus positive fetuses/newborns, 45% (34/76) presented with no signs/complications at birth, 20% (15/76) with moderate signs potentially related to CZS, 21% (16/76) with severe complications compatible with CZS, and 14% (11/76) with fetal loss. Compared with the Zika virus positive fetuses/neonates, those that were identified as negative for Zika virus (215/291) were less likely to present with severe complications (5%; 10/215) or fetal loss (0.5%; 1/215; relative risk 6.9, 95% confidence interval 3.6 to 13.3). Association between a positive Zika virus test and any adverse fetal/neonatal outcome was also significant (relative risk 4.4, 2.9 to 6.6). The population attributable fraction estimates that a confirmed congenital Zika virus infection contributes to 47% of adverse outcomes and 61% of severe adverse outcomes observed.
Conclusion: In cases of a known maternal Zika virus infection, approximately a quarter of fetuses will become congenitally infected, of which a third will have severe complications at birth or fetal loss. The burden of CZS might be lower than initially described in South America and may not differ from other congenital infections.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical