

Consistent effects of non-invasive vagus nerve stimulation (nVNS) for the acute treatment of migraine: additional findings from the randomized, sham-controlled, double-blind PRESTO trial
- PMID: 30382909
- PMCID: PMC6755599
- DOI: 10.1186/s10194-018-0929-0
Consistent effects of non-invasive vagus nerve stimulation (nVNS) for the acute treatment of migraine: additional findings from the randomized, sham-controlled, double-blind PRESTO trial
Erratum in
-
Correction to: Consistent effects of non-invasive vagus nerve stimulation (nVNS) for the acute treatment of migraine: additional findings from the randomized, sham-controlled, double-blind PRESTO trial.J Headache Pain. 2018 Dec 18;19(1):120. doi: 10.1186/s10194-018-0949-9. J Headache Pain. 2018. PMID: 30563446 Free PMC article.
Abstract
Background: Non-invasive vagus nerve stimulation (nVNS) has been shown to be practical, safe, and well tolerated for treating primary headache disorders. The recent multicenter, randomized, double-blind, sham-controlled PRESTO trial provided Class I evidence that for patients with episodic migraine, nVNS significantly increases the probability of having mild pain or being pain-free 2 h post stimulation. We report additional pre-defined secondary and other end points from PRESTO that demonstrate the consistency and durability of nVNS efficacy across a broad range of outcomes.
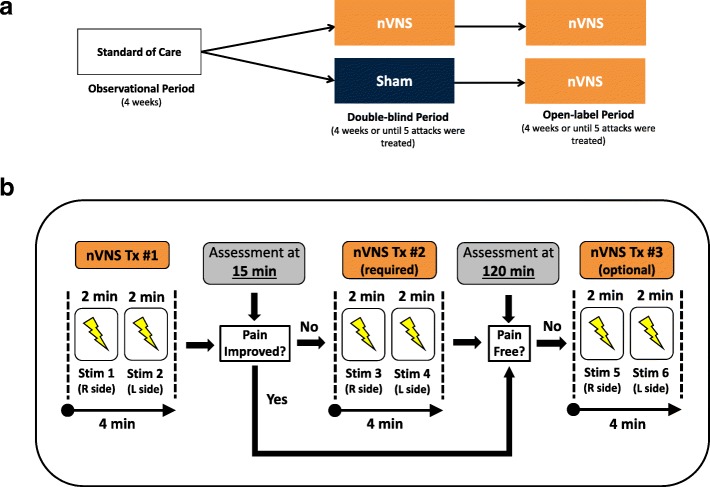
Methods: After a 4-week observation period, 248 patients with episodic migraine with/without aura were randomly assigned to acute treatment of migraine attacks with nVNS (n = 122) or a sham device (n = 126) during a double-blind period lasting 4 weeks (or until the patient had treated 5 attacks). All patients received nVNS therapy during the subsequent 4-week/5-attack open-label period.
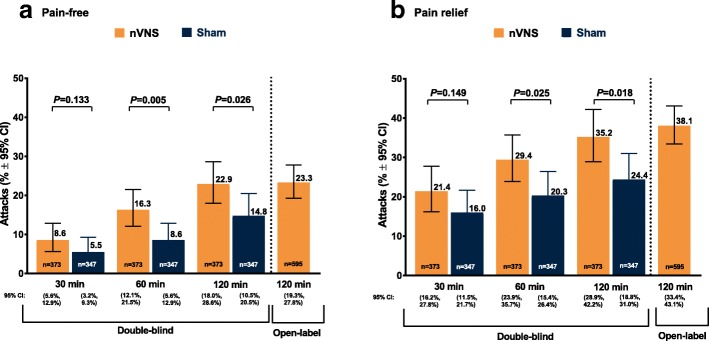
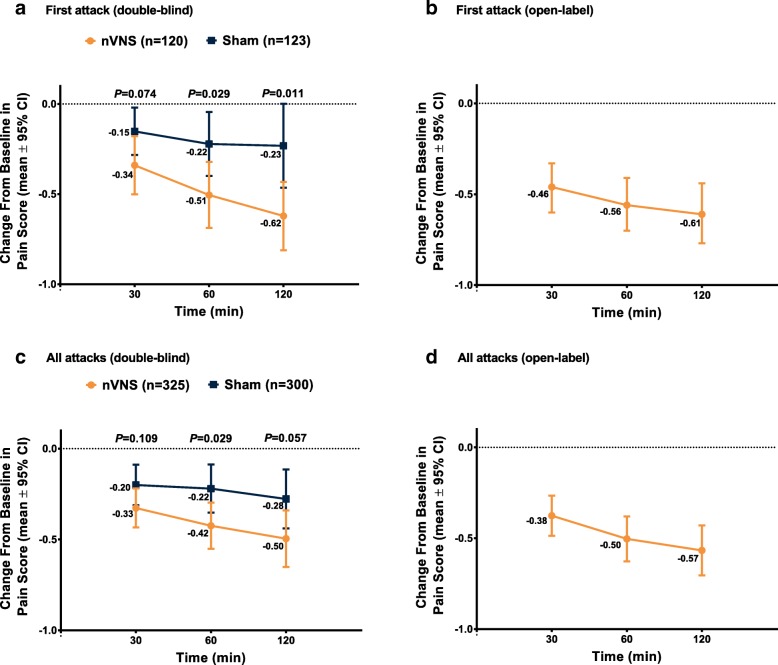
Results: The intent-to-treat population consisted of 243 patients. The nVNS group (n = 120) had a significantly greater percentage of attacks treated during the double-blind period that were pain-free at 60 (P = 0.005) and 120 min (P = 0.026) than the sham group (n = 123) did. Similar results were seen for attacks with pain relief at 60 (P = 0.025) and 120 min (P = 0.018). For the first attack and all attacks, the nVNS group had significantly greater decreases (vs sham) in pain score from baseline to 60 min (P = 0.029); the decrease was also significantly greater for nVNS at 120 min for the first attack (P = 0.011). Results during the open-label period were consistent with those of the nVNS group during the double-blind period. The incidence of adverse events (AEs) and adverse device effects was low across all study periods, and no serious AEs occurred.
Conclusions: These results further demonstrate that nVNS is an effective and reliable acute treatment for multiple migraine attacks, which can be used safely while preserving the patient's option to use traditional acute medications as rescue therapy, possibly decreasing the risk of medication overuse. Together with its practicality and optimal tolerability profile, these findings suggest nVNS has value as a front-line option for acute treatment of migraine.
Trial registration: ClinicalTrials.gov identifier: NCT02686034 .
Keywords: Double-blind; Migraine; Neuromodulation; Open-label; Pain intensity; Vagus nerve stimulation.
Conflict of interest statement
P. Martelletti has received research grants, advisory board fees, or travel fees from ACRAF; Allergan S.p.A.; Amgen Inc.; electroCore, Inc.; Novartis AG; and Teva Pharmaceutical Industries Ltd.
L. Grazzi has received consultancy and advisory fees from Allergan S.p.A. and electroCore, Inc.
G. Pierangeli has nothing to disclose.
I. Rainero has received consultancy fees from electroCore, Inc., and Mylan N.V. and research grants from the European Commission – Horizon 2020. He is also a principal investigator for RCTs sponsored by Axovant Sciences Ltd. and TauRx Pharmaceuticals Ltd.
P. Geppetti has received consultancy fees from Allergan S.p.A.; electroCore, Inc.; Evidera; Novartis AG; Pfizer Inc.; and Sanofi S.p.A. and research grants from Chiesi Farmaceutici S.p.A. He is also a principal investigator for RCTs sponsored by Eli Lilly and Company; Novartis AG; and Teva Pharmaceutical Industries Ltd.
A. Ambrosini has received consultancy fees from Almirall, S.A., and travel grants from Allergan S.p.A., Almirall, S.A., and Novartis.
P. Sarchielli has received clinical study fees from Allergan S.p.A.
P. Barbanti has received consultancy fees from Allergan S.p.A.; electroCore, Inc.; Janssen Pharmaceuticals, Inc.; Lusofarmaco; and Visufarma and advisory fees from Abbott Laboratories; Merck & Co., Inc.; Novartis AG; and Teva Pharmaceutical Industries Ltd. He is also a principal investigator for RCTs sponsored by Alder BioPharmaceuticals Inc.; Eli Lilly and Company; GlaxoSmithKline Pharmaceuticals Ltd.; and Teva Pharmaceutical Industries Ltd.
C. Tassorelli has consulted for Allergan S.p.A.; electroCore, Inc.; Eli Lilly and Company; and Novartis AG and has received research grants from the European Commission and the Italian Ministry of Health. She is also a principal investigator or collaborator for RCTs sponsored by Alder BioPharmaceuticals Inc.; Eli Lilly and Company; Novartis; and Teva Pharmaceutical Industries Ltd.
E. Liebler is an employee of electroCore, Inc., and receives stock ownership.
M. de Tommaso has received advisory fees from Allergan S.p.A.; Neopharmed; and Pfizer Inc.
Figures
References
-
- Lopes M, Dunn JD, Calhoun AH, Rapoport AM. Concepts in acute migraine management: clinical and managed care perspectives. Am J Pharm Benefits. 2012;4(5):201–206.
