Engaging Diverse English- and Spanish-Speaking Older Adults in Advance Care Planning: The PREPARE Randomized Clinical Trial
- PMID: 30383086
- PMCID: PMC6342283
- DOI: 10.1001/jamainternmed.2018.4657
Engaging Diverse English- and Spanish-Speaking Older Adults in Advance Care Planning: The PREPARE Randomized Clinical Trial
Abstract
Importance: Advance care planning improves the receipt of medical care aligned with patients' values; however, it remains suboptimal among diverse patient populations. To mitigate literacy, cultural, and language barriers to advance care planning, easy-to-read advance directives and a patient-directed, online advance care planning program called PREPARE For Your Care (PREPARE) were created in English and Spanish.
Objective: To compare the efficacy of PREPARE plus an easy-to-read advance directive with an advance directive alone to increase advance care planning documentation and patient-reported engagement.
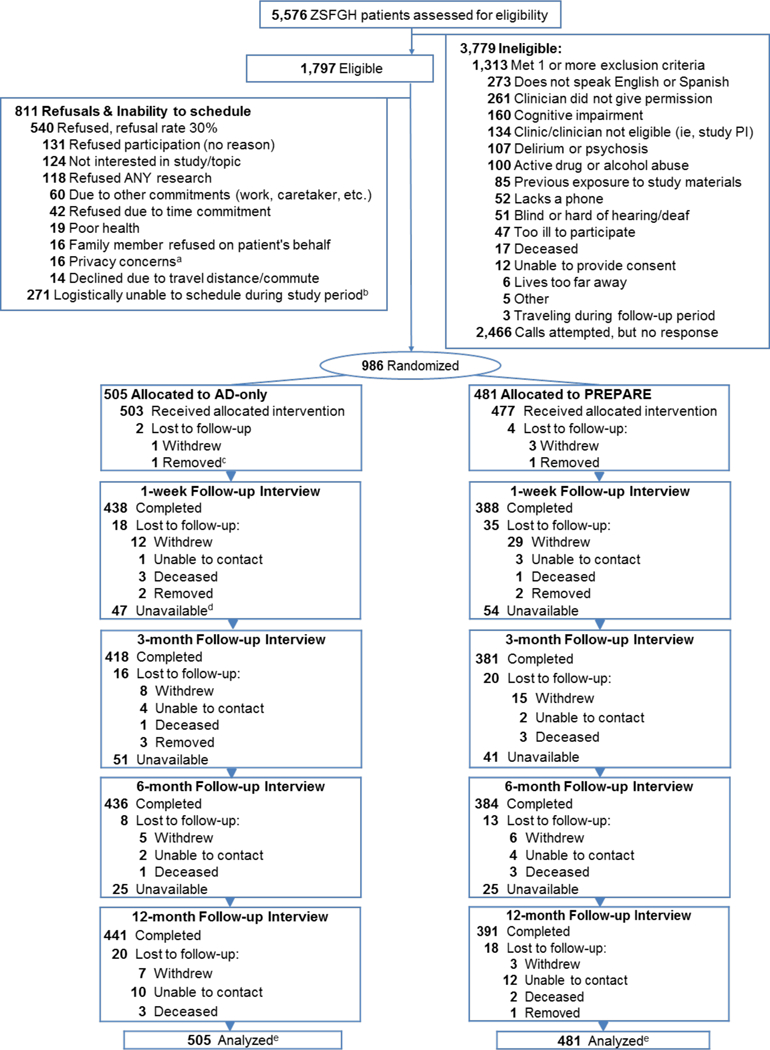
Design, setting, and participants: A comparative efficacy randomized clinical trial was conducted from February 1, 2014, to November 30, 2017, at 4 safety-net, primary-care clinics in San Francisco among 986 English-speaking or Spanish-speaking primary care patients 55 years or older with 2 or more chronic or serious illnesses.
Interventions: Participants were randomized to PREPARE plus an easy-to-read advance directive (PREPARE arm) or the advance directive alone. There were no clinician-level or system-level interventions. Staff were blinded for all follow-up measurements.
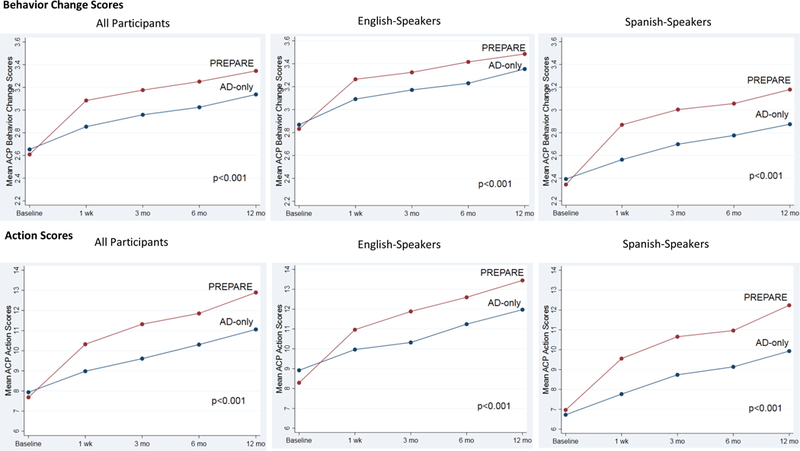
Main outcomes and measures: The primary outcome was documentation of new advance care planning (ie, legal forms and/or documented discussions) at 15 months. Patient-reported outcomes included advance care planning engagement at baseline, 1 week, 3 months, 6 months, and 12 months using validated surveys. Intention-to-treat analyses were performed using mixed-effects logistic and linear regression, controlling for time, health literacy, and baseline advance care planning, clustering by physician, and stratifying by language.
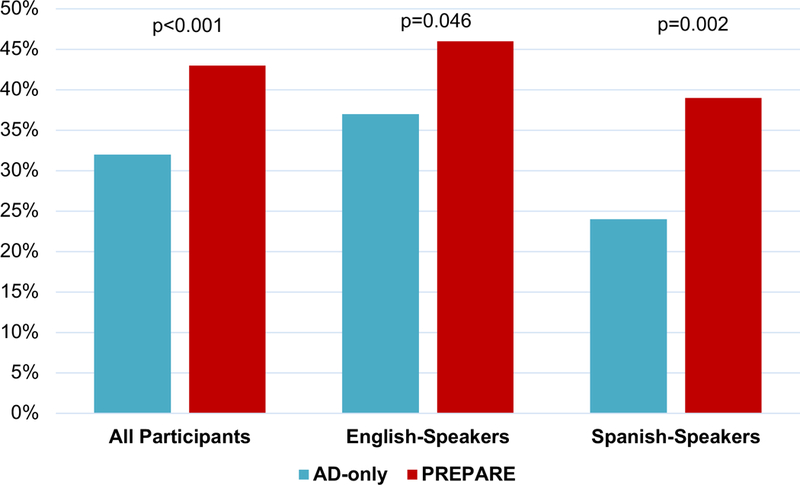
Results: Among the 986 participants (603 women and 383 men), the mean (SD) age was 63.3 (6.4) years, 387 of 975 (39.7%) had limited health literacy, and 445 (45.1%) were Spanish speaking. No participant characteristic differed between the 2 groups, and retention was 85.9% (832 of 969) among survivors. Compared with the advance directive alone, PREPARE resulted in a higher rate of advance care planning documentation (unadjusted, 43.0% [207 of 481] vs 33.1% [167 of 505]; P < .001; adjusted, 43.0% vs 32.0%; P < .001) and higher self-reported increased advance care planning engagement scores (98.1% vs 89.5%; P < .001). Results remained significant among English speakers and Spanish speakers.
Conclusions and relevance: The patient-facing PREPARE program and an easy-to-read advance directive, without clinician-level or system-level interventions, increased documentation of advance care planning and patient-reported engagement, with statistically higher gains for PREPARE vs advance directive alone. These tools may mitigate literacy and language barriers to advance care planning, allow patients to begin planning on their own, and could substantially improve the process for diverse English-speaking and Spanish-speaking populations.
Trial registration: ClinicalTrials.gov identifiers: NCT01990235 and NCT02072941.
Conflict of interest statement
Figures