

Interventions for Preventing Thromboembolic Events in Patients With Atrial Fibrillation: A Systematic Review
- PMID: 30383133
- PMCID: PMC6825839
- DOI: 10.7326/M18-1523
Interventions for Preventing Thromboembolic Events in Patients With Atrial Fibrillation: A Systematic Review
Abstract
Background: The comparative safety and effectiveness of treatments to prevent thromboembolic complications in atrial fibrillation (AF) remain uncertain.
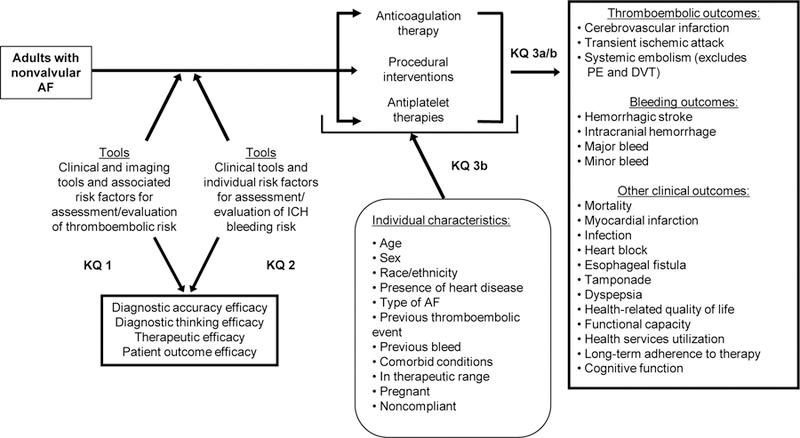
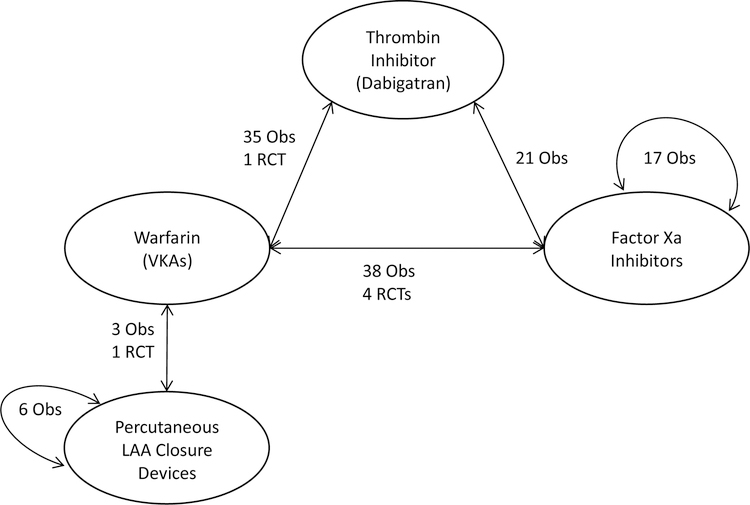
Purpose: To compare the effectiveness of medical and procedural therapies in preventing thromboembolic events and bleeding complications in adults with nonvalvular AF.
Data sources: English-language studies in several databases from 1 January 2000 to 14 February 2018.
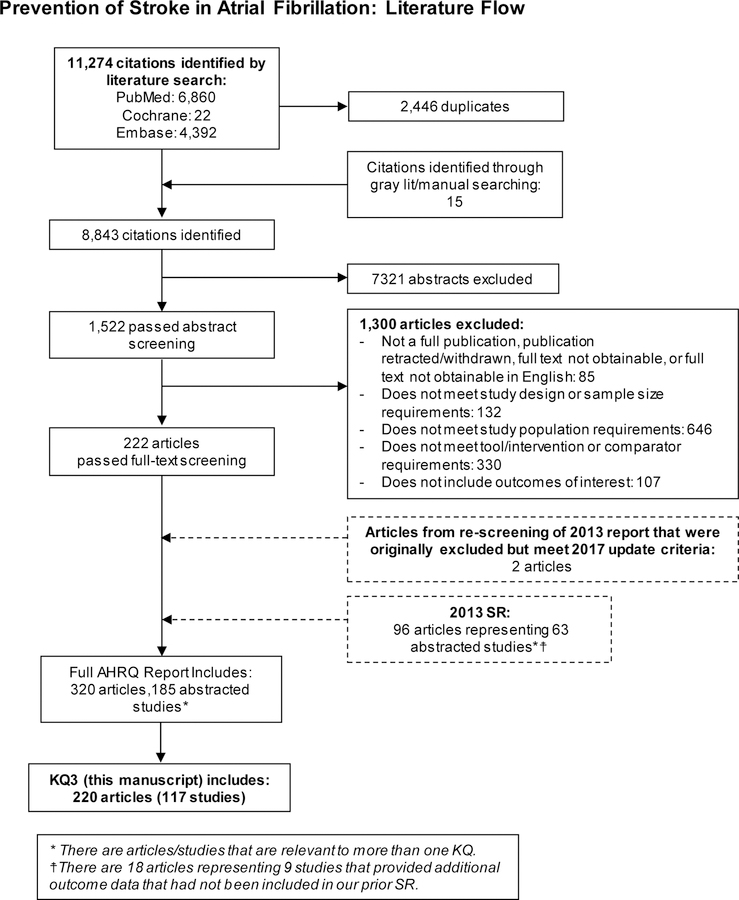
Study selection: Two reviewers independently screened citations to identify comparative studies of treatments to prevent stroke in adults with nonvalvular AF who reported thromboembolic or bleeding complications.
Data extraction: Two reviewers independently abstracted data, assessed study quality and applicability, and rated strength of evidence.
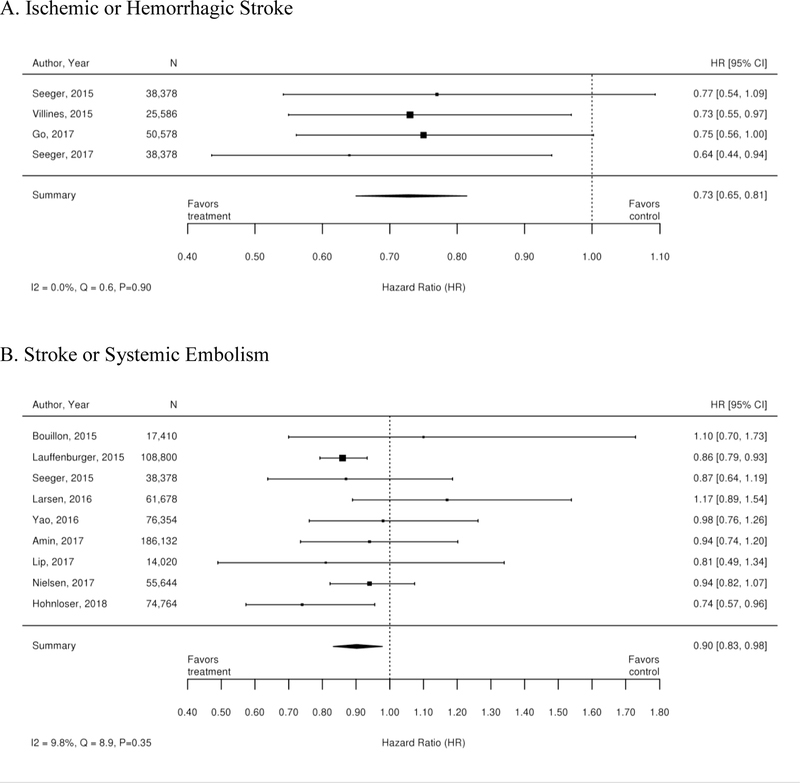
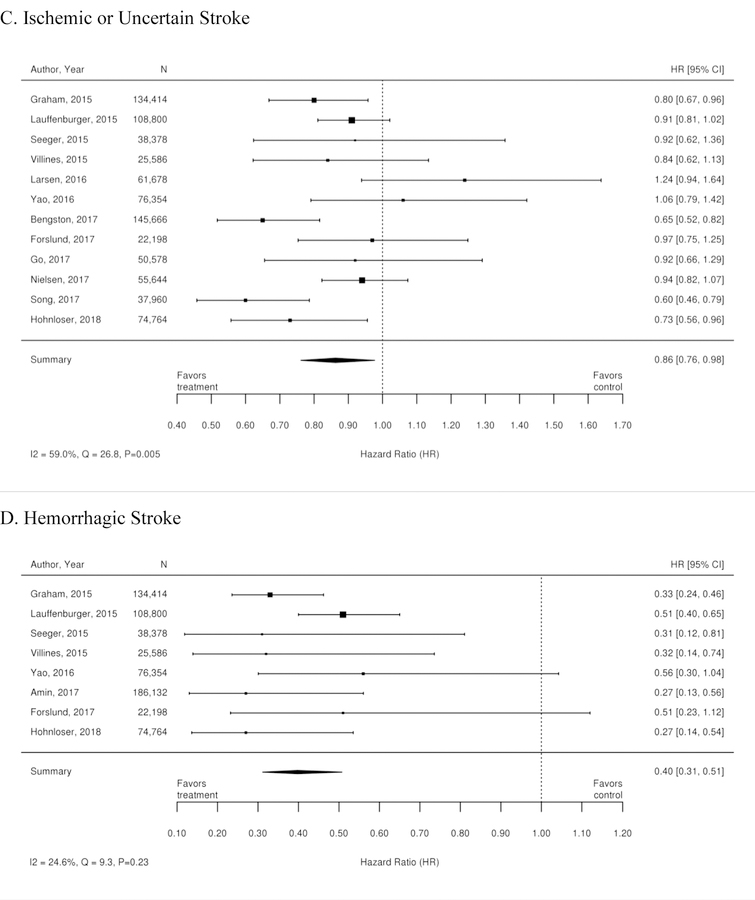
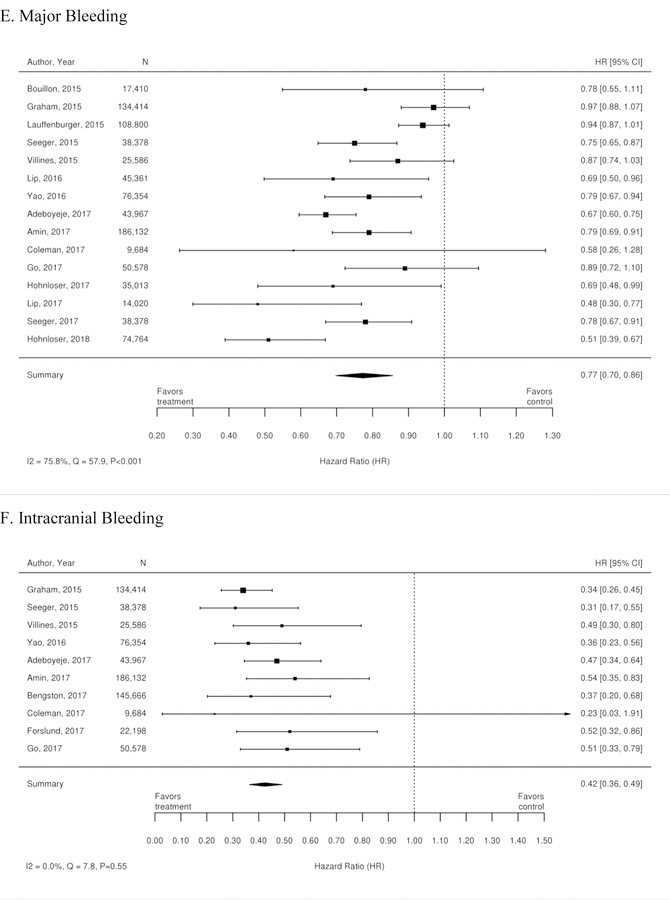
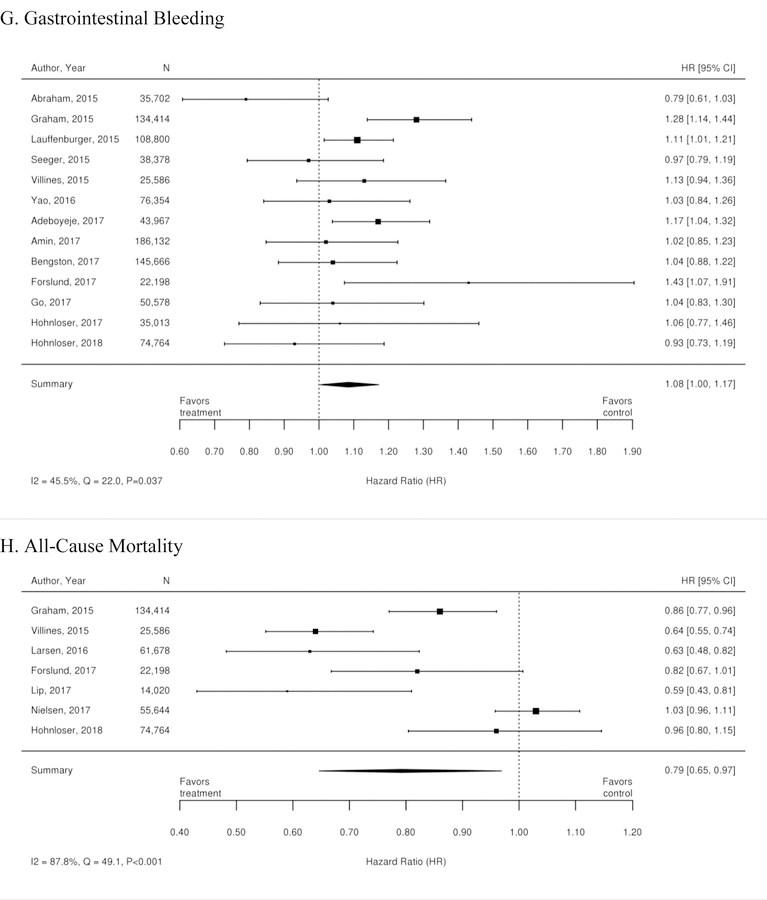
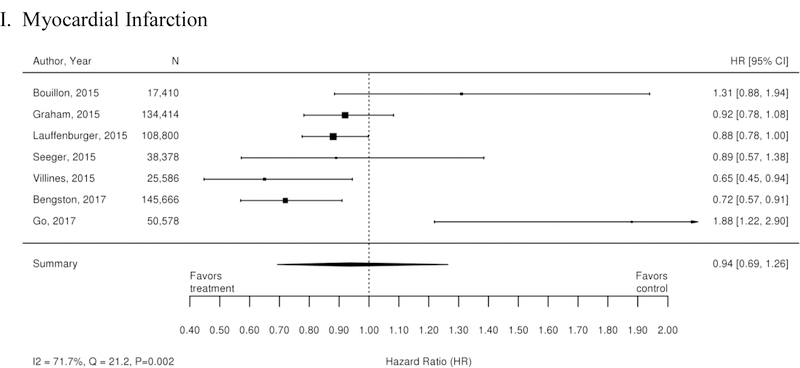
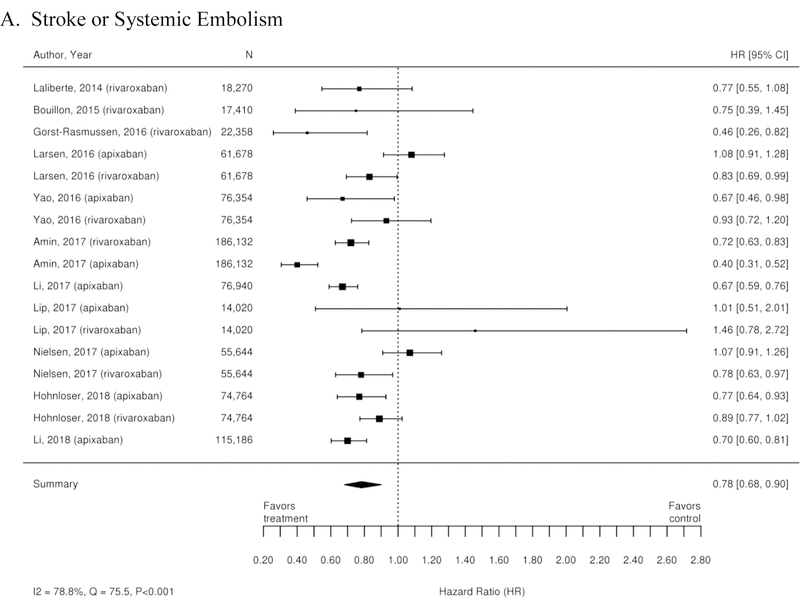
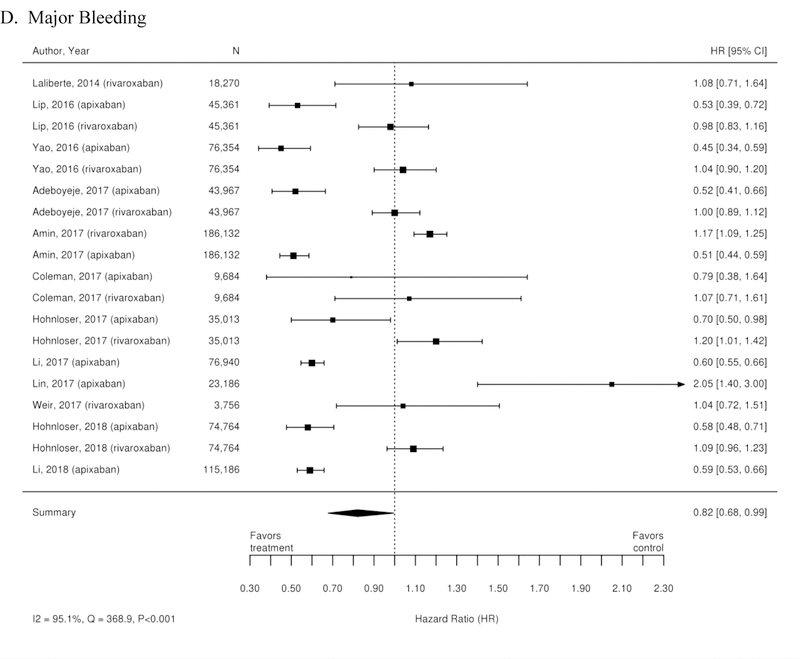
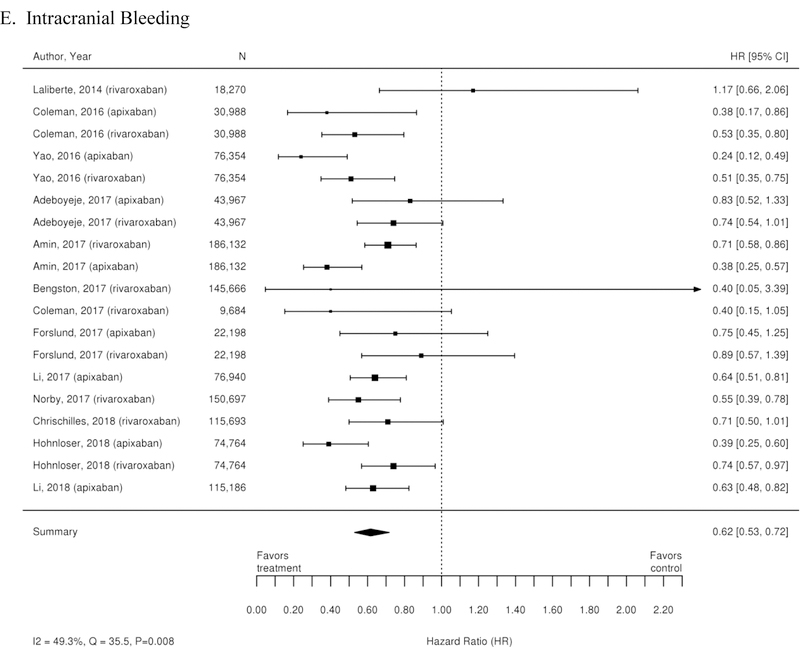
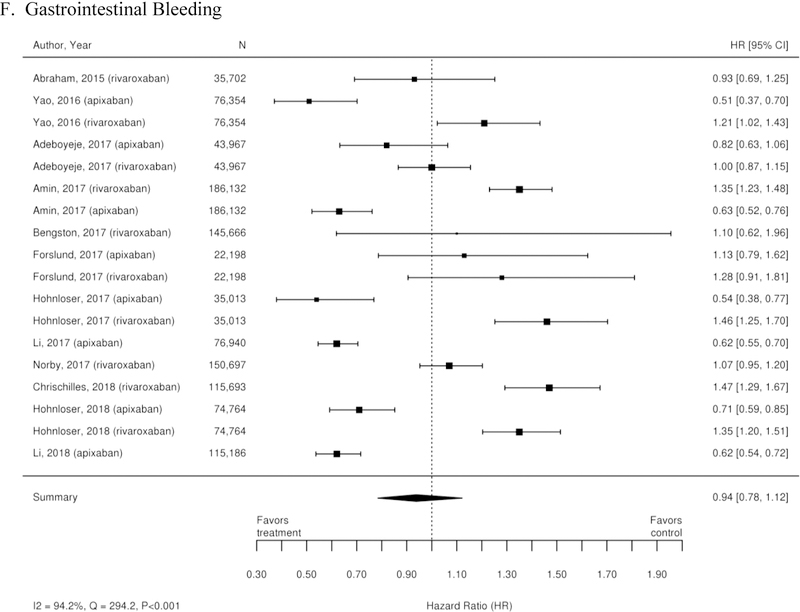
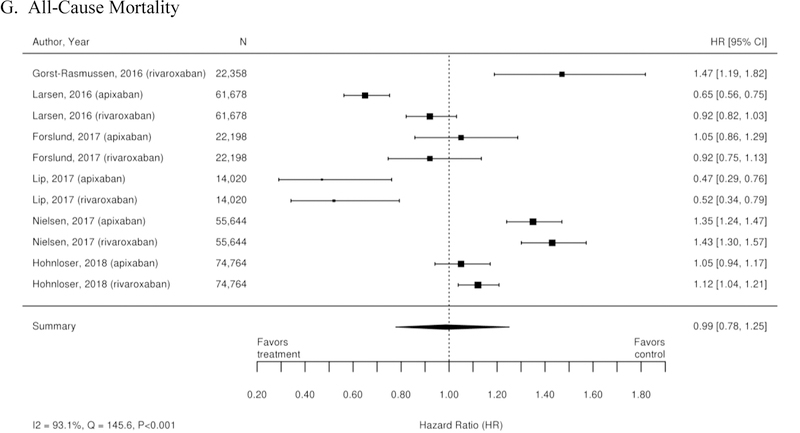
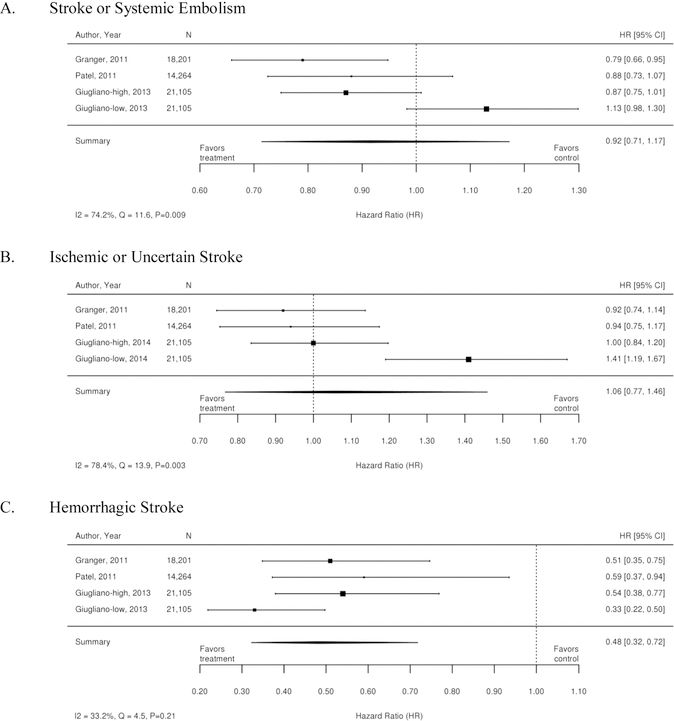
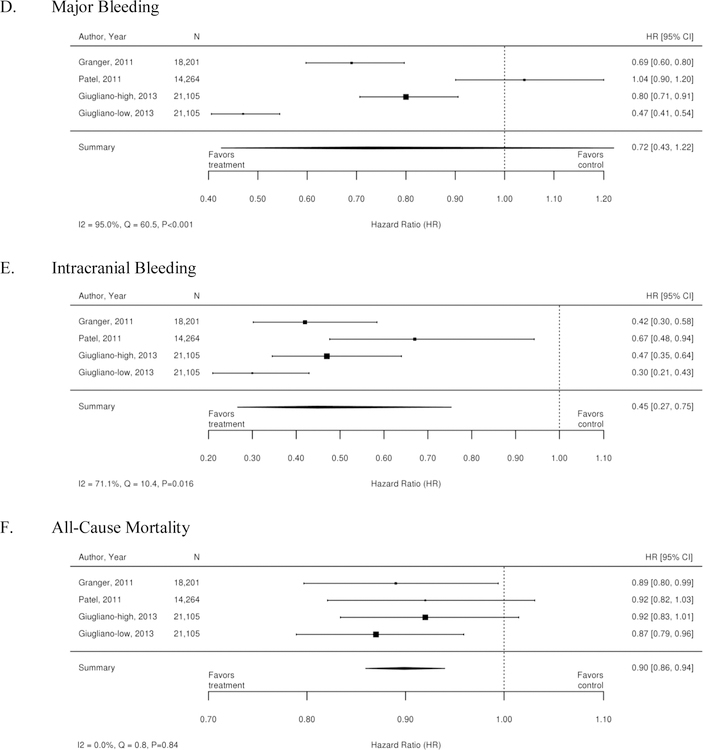
Data synthesis: Data from 220 articles were included. Dabigatran and apixaban were superior and rivaroxaban and edoxaban were similar to warfarin in preventing stroke or systemic embolism. Apixaban and edoxaban were superior and rivaroxaban and dabigatran were similar to warfarin in reducing the risk for major bleeding. Treatment effects with dabigatran were similar in patients with renal dysfunction (interaction P > 0.05), and patients younger than 75 years had lower bleeding rates with dabigatran (interaction P < 0.001). The benefit of treatment with apixaban was consistent in many subgroups, including those with renal impairment, diabetes, and prior stroke (interaction P > 0.05 for all). The greatest bleeding risk reduction was observed in patients with a glomerular filtration rate less than 50 mL/min/1.73 m2 (P = 0.003). Similar treatment effects were observed for rivaroxaban and edoxaban in patients with prior stroke, diabetes, or heart failure (interaction P > 0.05 for all).
Limitation: Heterogeneous study populations, interventions, and outcomes.
Conclusion: The available direct-acting oral anticoagulants (DOACs) are at least as effective and safe as warfarin for patients with nonvalvular AF. The DOACs had similar benefits across several patient subgroups and seemed safe and efficacious for a wide range of patients with nonvalvular AF.
Primary funding source: Patient-Centered Outcomes Research Institute. (PROSPERO: CRD42017069999).
Figures
References
-
- Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, et al. ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006;114(7):e257–354. - PubMed
-
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114(2):119–25. - PubMed
-
- Thrall G, Lane D, Carroll D, Lip GY. Quality of life in patients with atrial fibrillation: a systematic review. Am J Med. 2006;119(5):448 e1–19. - PubMed
-
- Stewart S, Hart CL, Hole DJ, McMurray JJ. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am J Med. 2002;113(5):359–64. - PubMed
-
- Lee WC, Lamas GA, Balu S, Spalding J, Wang Q, Pashos CL. Direct treatment cost of atrial fibrillation in the elderly American population: a Medicare perspective. J Med Econ. 2008;11(2):281–98. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical