

Prevalence and Changes in Preexisting Diabetes and Gestational Diabetes Among Women Who Had a Live Birth - United States, 2012-2016
- PMID: 30383743
- PMCID: PMC6319799
- DOI: 10.15585/mmwr.mm6743a2
Prevalence and Changes in Preexisting Diabetes and Gestational Diabetes Among Women Who Had a Live Birth - United States, 2012-2016
Abstract
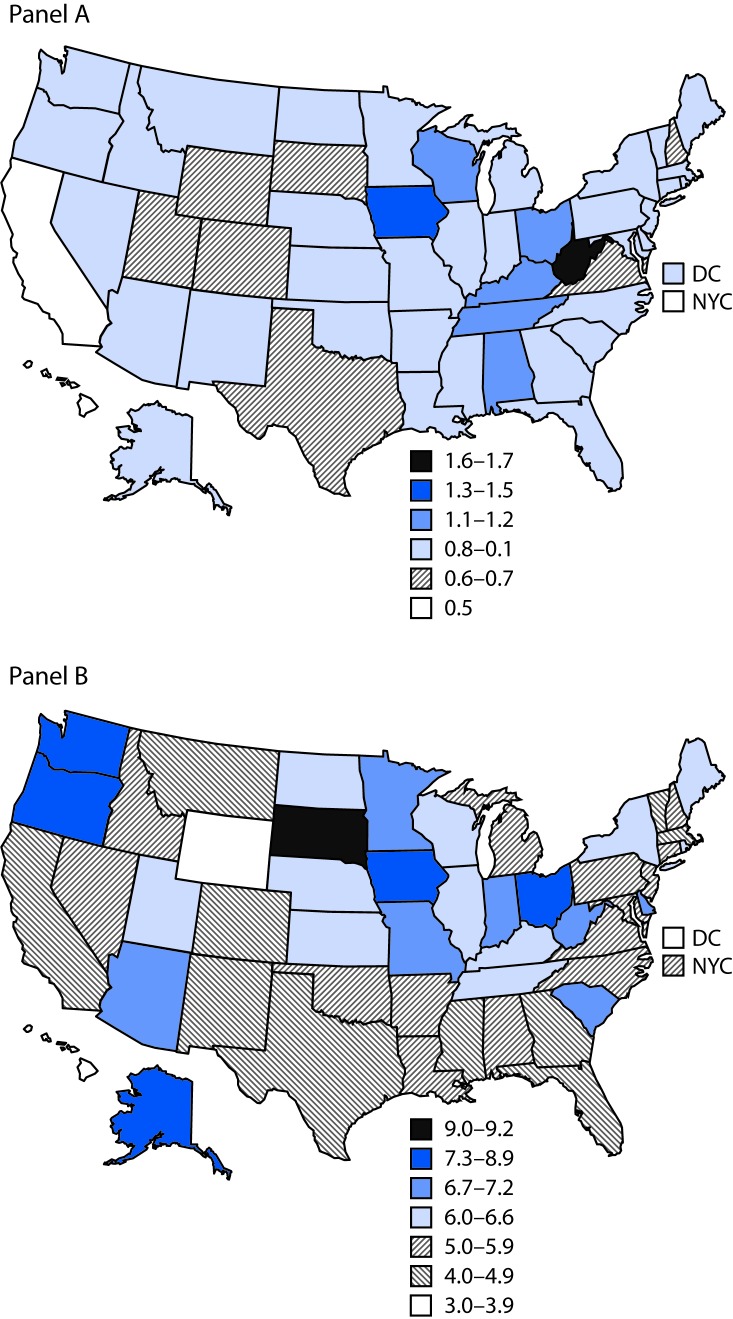
Diabetes during pregnancy increases the risk for adverse maternal and infant health outcomes. Type 1 or type 2 diabetes diagnosed before pregnancy (preexisting diabetes) increases infants' risk for congenital anomalies, stillbirth, and being large for gestational age (1). Diabetes that develops and is diagnosed during the second half of pregnancy (gestational diabetes) increases infants' risk for being large for gestational age (1) and might increase the risk for childhood obesity (2); for mothers, gestational diabetes increases the risk for future type 2 diabetes (3). In the United States, prevalence of both preexisting and gestational diabetes increased from 2000 to 2010 (4,5). Recent state-specific trends have not been reported; therefore, CDC analyzed 2012-2016 National Vital Statistics System (NVSS) birth data. In 2016, the crude national prevalence of preexisting diabetes among women with live births was 0.9%, and prevalence of gestational diabetes was 6.0%. Among 40 jurisdictions with continuously available data from 2012 through 2016, the age- and race/ethnicity-standardized prevalence of preexisting diabetes was stable at 0.8% and increased slightly from 5.2% to 5.6% for gestational diabetes. Preconception care and lifestyle interventions before, during, and after pregnancy might provide opportunities to control, prevent, or mitigate health risks associated with diabetes during pregnancy.
Conflict of interest statement
All authors have completed and submitted the ICMJE form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
