

Reasons for Discontinuing Active Surveillance: Assessment of 21 Centres in 12 Countries in the Movember GAP3 Consortium
- PMID: 30385049
- PMCID: PMC8542419
- DOI: 10.1016/j.eururo.2018.10.025
Reasons for Discontinuing Active Surveillance: Assessment of 21 Centres in 12 Countries in the Movember GAP3 Consortium
Abstract
Background: Careful assessment of the reasons for discontinuation of active surveillance (AS) is required for men with prostate cancer (PCa).
Objective: Using Movember's Global Action Plan Prostate Cancer Active Surveillance initiative (GAP3) database, we report on reasons for AS discontinuation.
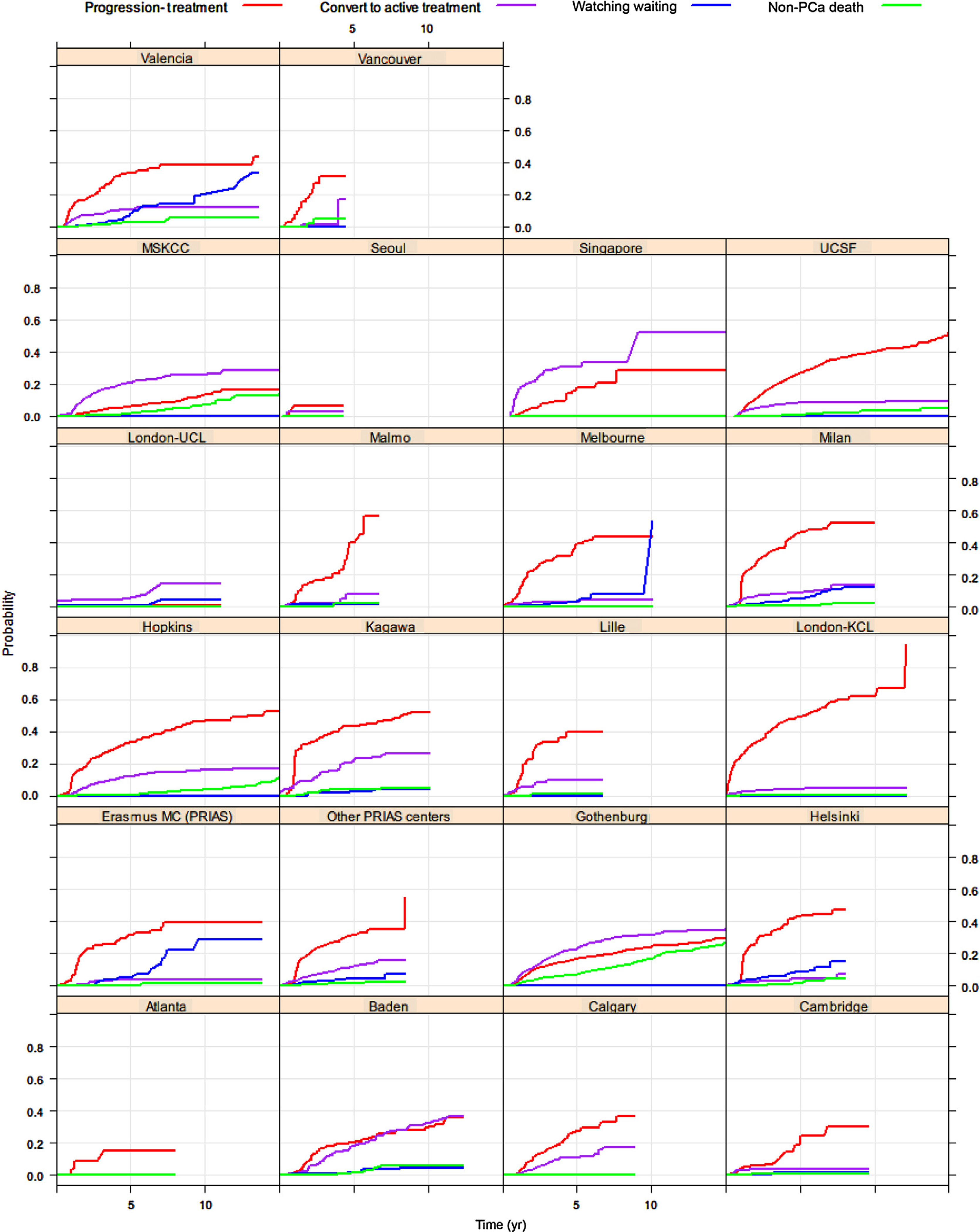
Design, setting, and participants: We compared data from 10296 men on AS from 21 centres across 12 countries.
Outcome measurements and statistical analysis: Cumulative incidence methods were used to estimate the cumulative incidence rates of AS discontinuation.
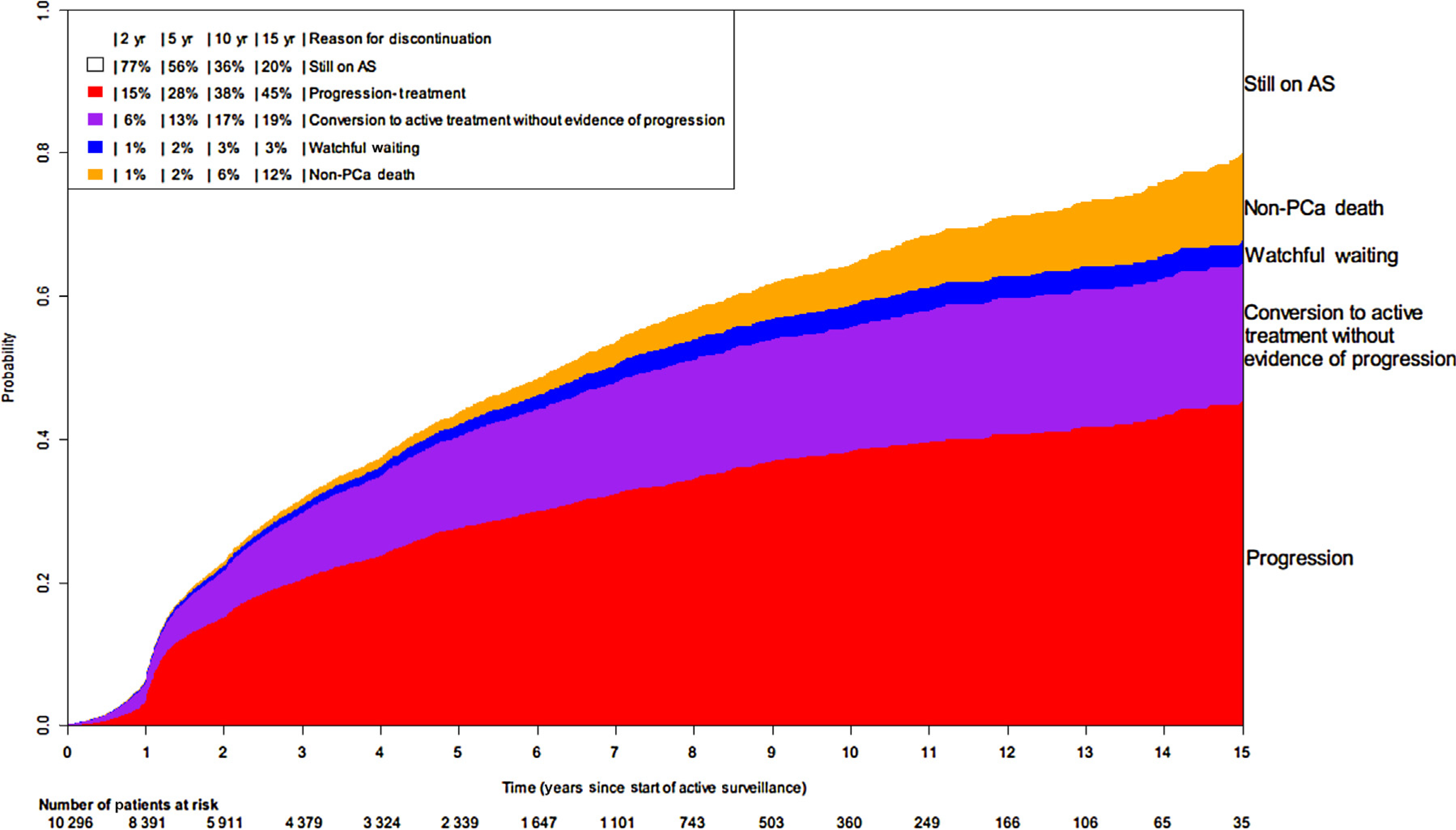
Results and limitations: During 5-yr follow-up, 27.5% (95% confidence interval [CI]: 26.4-28.6%) men showed signs of disease progression, 12.8% (95% CI: 12.0-13.6%) converted to active treatment without evidence of progression, 1.7% (95% CI: 1.5-2.0%) continued to watchful waiting, and 1.7% (95% CI: 1.4-2.1%) died from other causes. Of the 7049 men who remained on AS, 2339 had follow-up for >5yr, 4561 had follow-up for <5yr, and 149 were lost to follow-up. Cumulative incidence of progression was 27.5% (95% CI: 26.4-28.6%) at 5yr and 38.2% (95% CI: 36.7-39.9%) at 10yr. A limitation is that not all centres were included due to limited information on the reason for discontinuation and limited follow-up.
Conclusions: Our descriptive analyses of current AS practices worldwide showed that 43.6% of men drop out of AS during 5-yr follow-up, mainly due to signs of disease progression. Improvements in selection tools for AS are thus needed to correctly allocate men with PCa to AS, which will also reduce discontinuation due to conversion to active treatment without evidence of disease progression.
Patient summary: Our assessment of a worldwide database of men with prostate cancer (PCa) on active surveillance (AS) shows that 43.6% drop out of AS within 5yr, mainly due to signs of disease progression. Better tools are needed to select and monitor men with PCa as part of AS.
Keywords: Active surveillance; Discontinuation; Prostate cancer; Worldwide.
Copyright © 2018 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Re: Reasons for Discontinuing Active Surveillance: Assessment of 21 Centres in 12 Countries in the Movember GAP3 Consortium.J Urol. 2020 Feb;203(2):252-253. doi: 10.1097/JU.0000000000000648. Epub 2019 Nov 11. J Urol. 2020. PMID: 31710568 No abstract available.
References
-
- Albertsen PC. Active surveillance: a ten-year journey. Eur Urol 2017;72:542–3. - PubMed
-
- Dall’Era MA, Albertsen PC, Bangma C, et al. Active surveillance for prostate cancer: a systematic review of the literature. Eur Urol 2012;62:976–83. - PubMed
-
- Bokhorst LP, Alberts AR, Rannikko A, et al. Compliance rates with the Prostate Cancer Research International Active Surveillance (PRIAS) protocol and disease reclassification in noncompliers. Eur Urol 2015;68:814–21. - PubMed
-
- Bruinsma SM, Bangma CH, Carroll PR, et al. Active surveillance for prostate cancer: a narrative review of clinical guidelines. Nat Rev Urol 2016;13:151–67. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
