

Dietary protein restriction reduces circulating VLDL triglyceride levels via CREBH-APOA5-dependent and -independent mechanisms
- PMID: 30385734
- PMCID: PMC6238732
- DOI: 10.1172/jci.insight.99470
Dietary protein restriction reduces circulating VLDL triglyceride levels via CREBH-APOA5-dependent and -independent mechanisms
Abstract
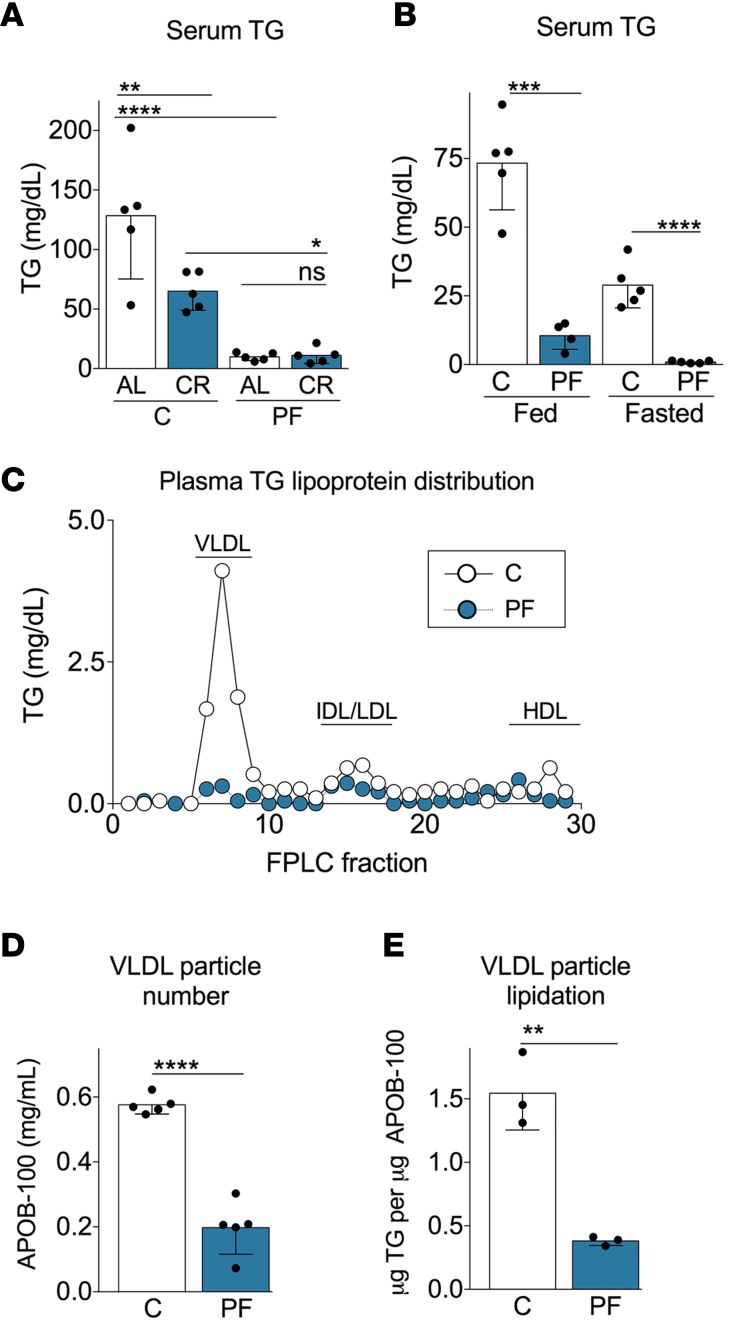
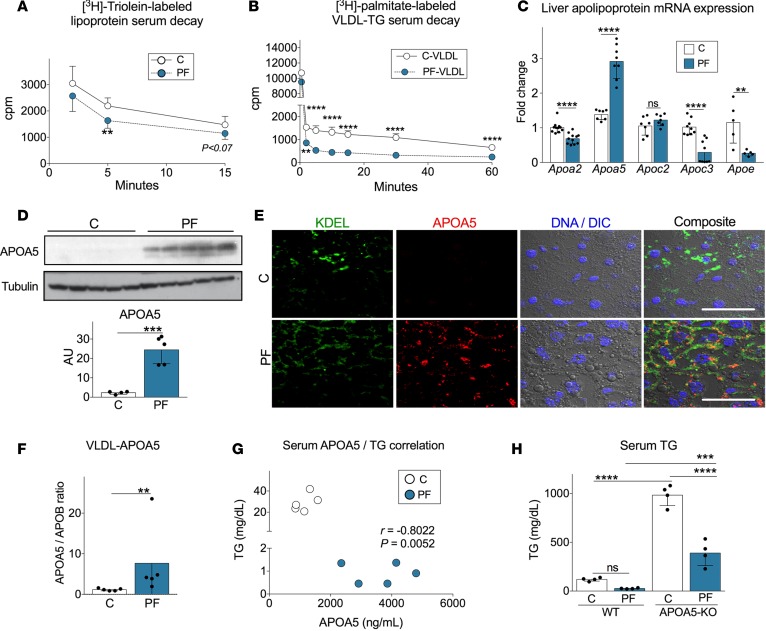
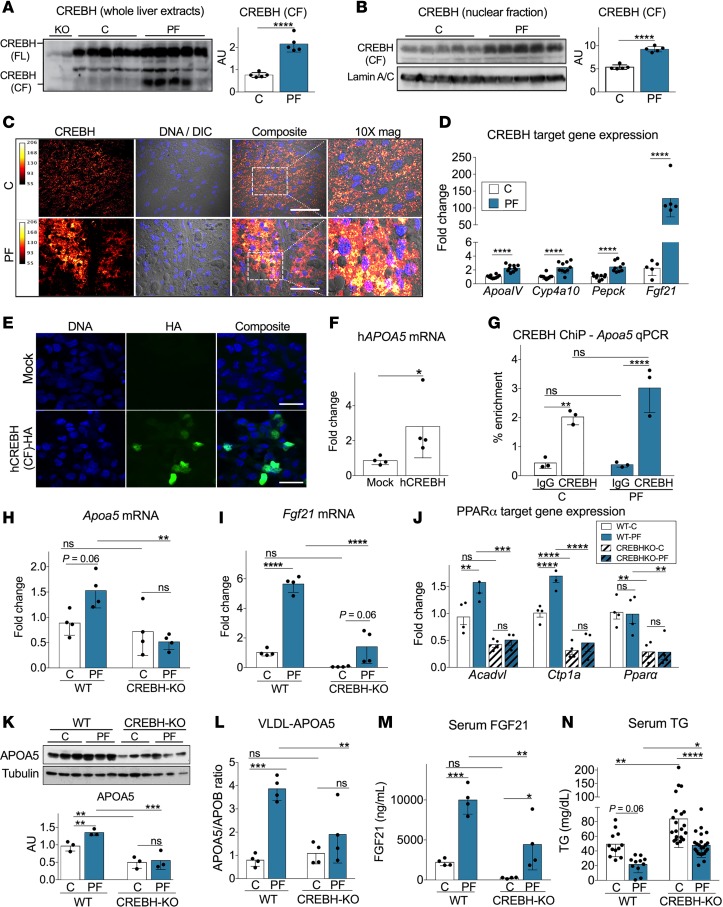
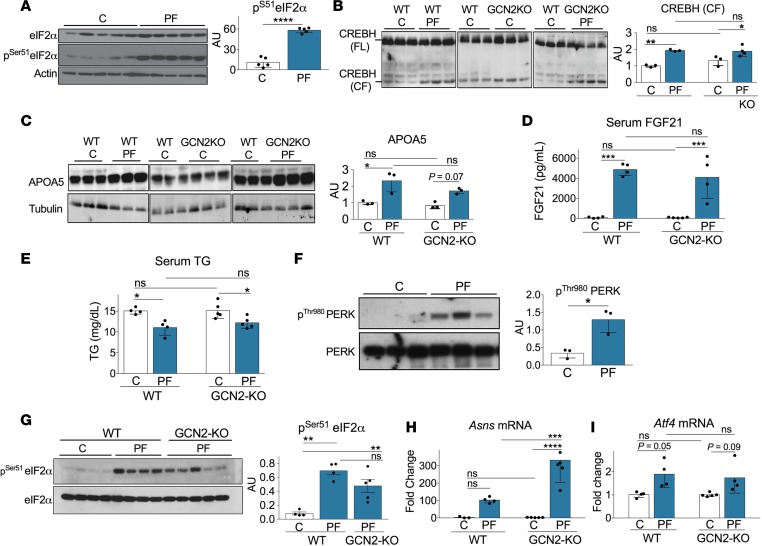
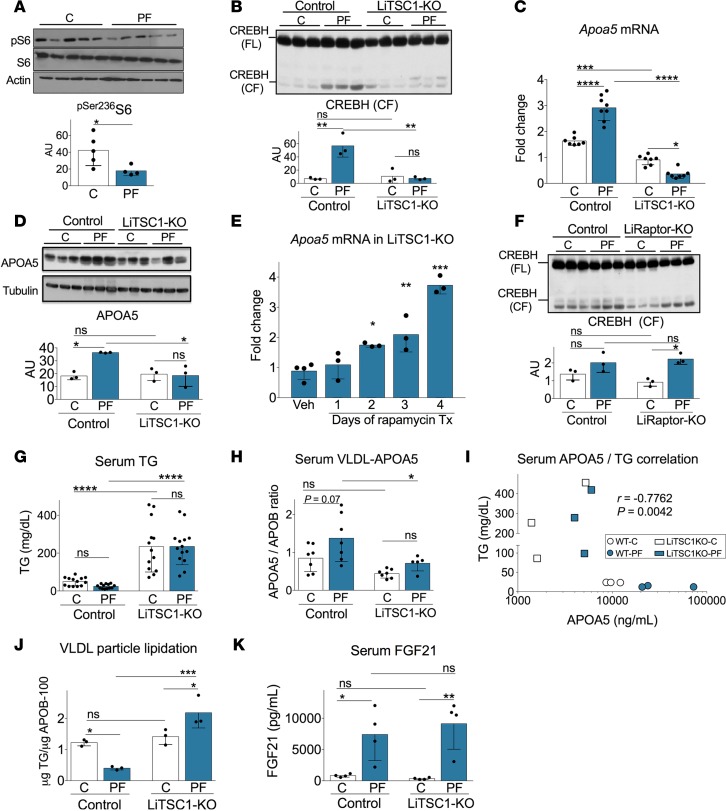
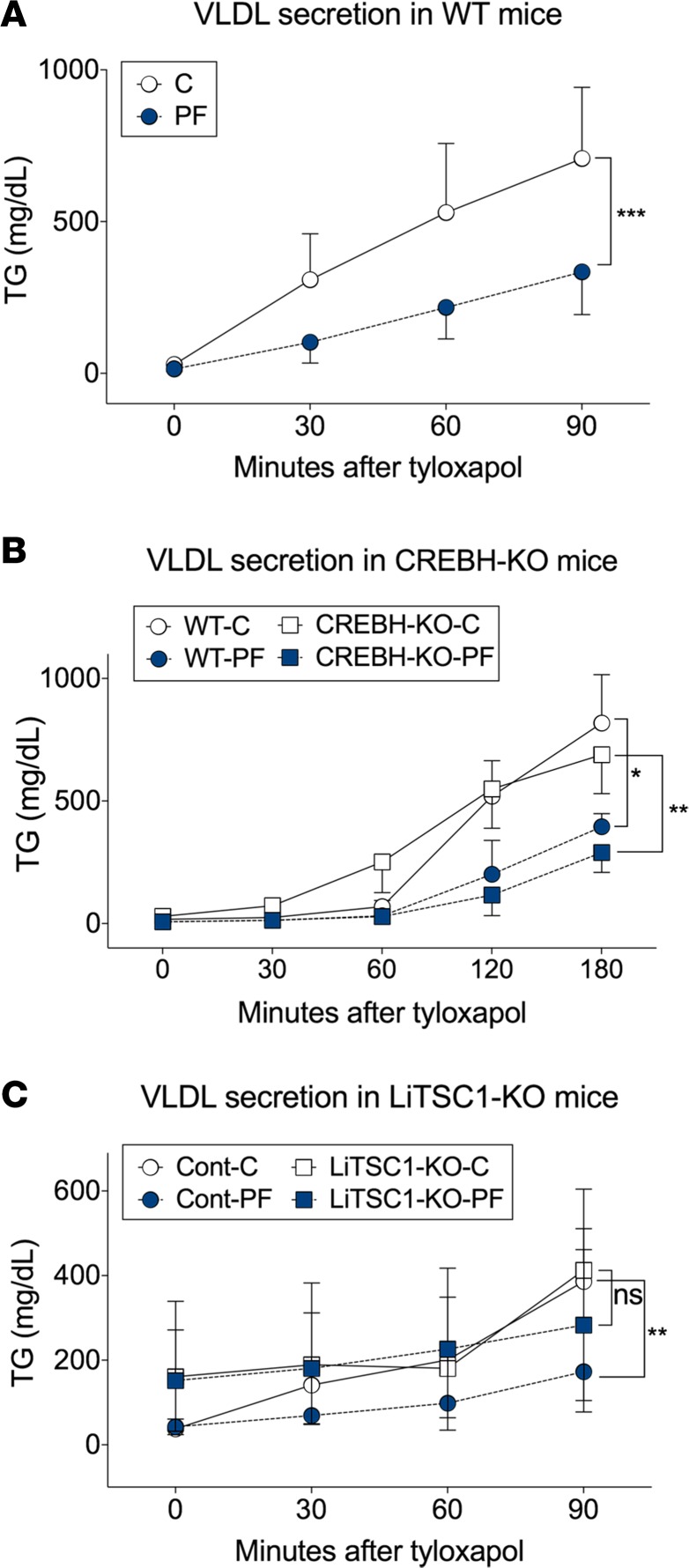
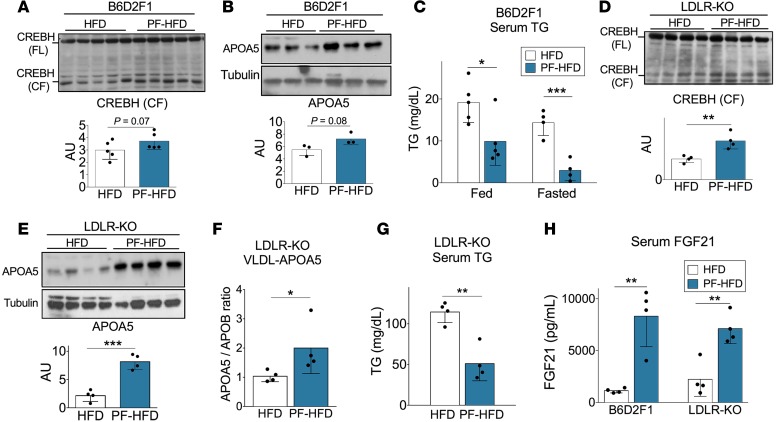
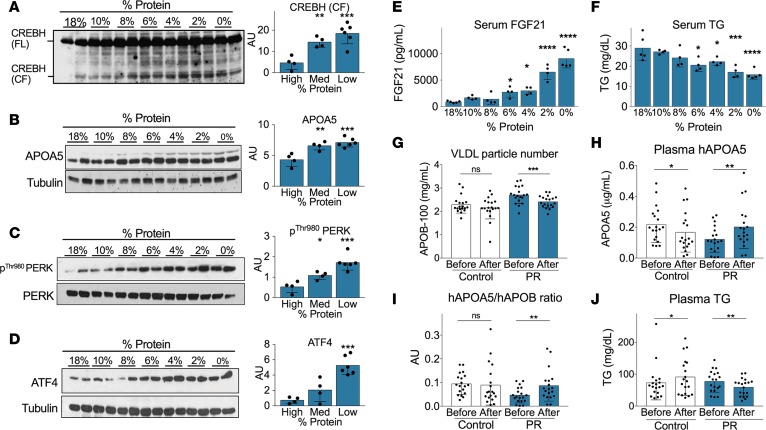
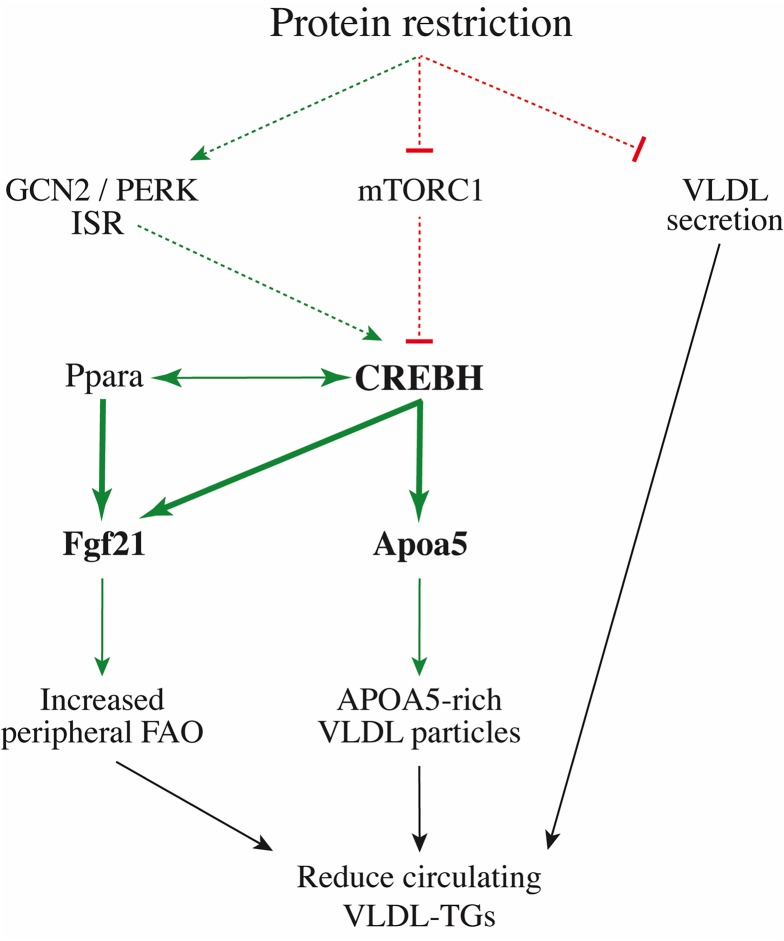
Hypertriglyceridemia is an independent risk factor for cardiovascular disease. Dietary interventions based on protein restriction (PR) reduce circulating triglycerides (TGs), but underlying mechanisms and clinical relevance remain unclear. Here, we show that 1 week of a protein-free diet without enforced calorie restriction significantly lowered circulating TGs in both lean and diet-induced obese mice. Mechanistically, the TG-lowering effect of PR was due, in part, to changes in very low-density lipoprotein (VLDL) metabolism both in liver and peripheral tissues. In the periphery, PR stimulated VLDL-TG consumption by increasing VLDL-bound APOA5 expression and promoting VLDL-TG hydrolysis and clearance from circulation. The PR-mediated increase in Apoa5 expression was controlled by the transcription factor CREBH, which coordinately regulated hepatic expression of fatty acid oxidation-related genes, including Fgf21 and Ppara. The CREBH-APOA5 axis activation upon PR was intact in mice lacking the GCN2-dependent amino acid-sensing arm of the integrated stress response. However, constitutive hepatic activation of the amino acid-responsive kinase mTORC1 compromised CREBH activation, leading to blunted APOA5 expression and PR-recalcitrant hypertriglyceridemia. PR also contributed to hypotriglyceridemia by reducing the rate of VLDL-TG secretion, independently of activation of the CREBH-APOA5 axis. Finally, a randomized controlled clinical trial revealed that 4-6 weeks of reduced protein intake (7%-9% of calories) decreased VLDL particle number, increased VLDL-bound APOA5 expression, and lowered plasma TGs, consistent with mechanistic conservation of PR-mediated hypotriglyceridemia in humans with translational potential as a nutraceutical intervention for dyslipidemia.
Keywords: Lipoproteins; Metabolism.
Conflict of interest statement
Figures
References
-
- Hokanson JE, Austin MA. Plasma triglyceride level is a risk factor for cardiovascular disease independent of high-density lipoprotein cholesterol level: a meta-analysis of population-based prospective studies. J Cardiovasc Risk. 1996;3(2):213–219. doi: 10.1097/00043798-199604000-00014. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
