

The Dual Burden of Malnutrition Increases the Risk of Cesarean Delivery: Evidence From India
- PMID: 30386761
- PMCID: PMC6199394
- DOI: 10.3389/fpubh.2018.00292
The Dual Burden of Malnutrition Increases the Risk of Cesarean Delivery: Evidence From India
Abstract
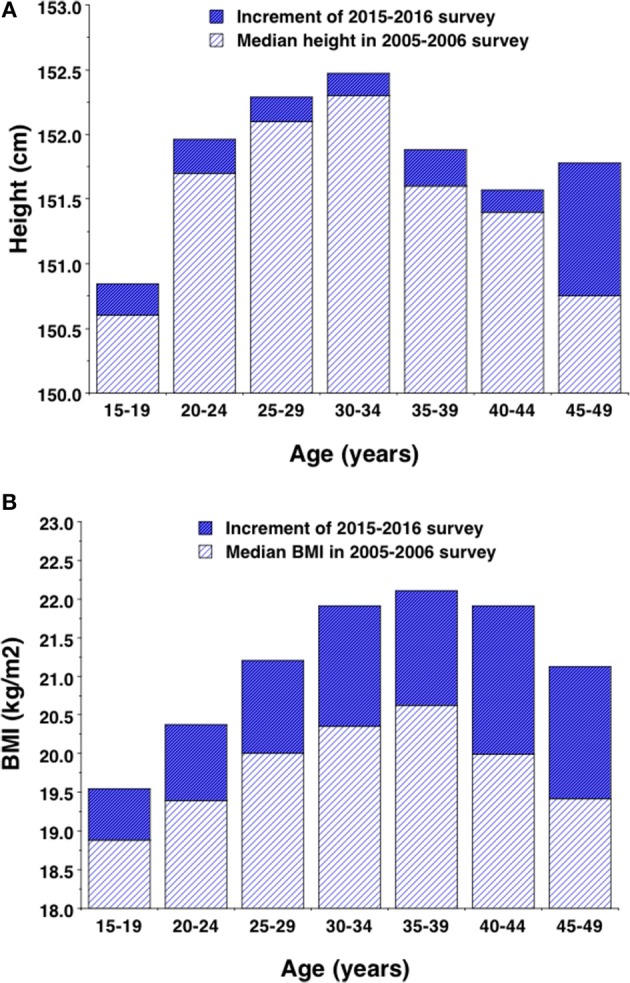
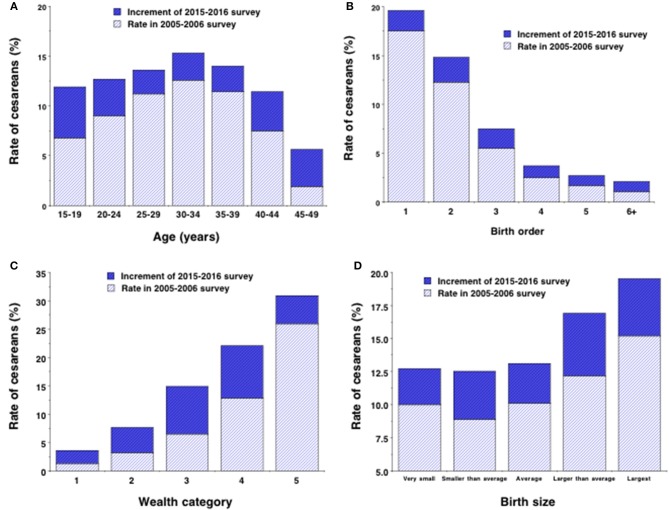
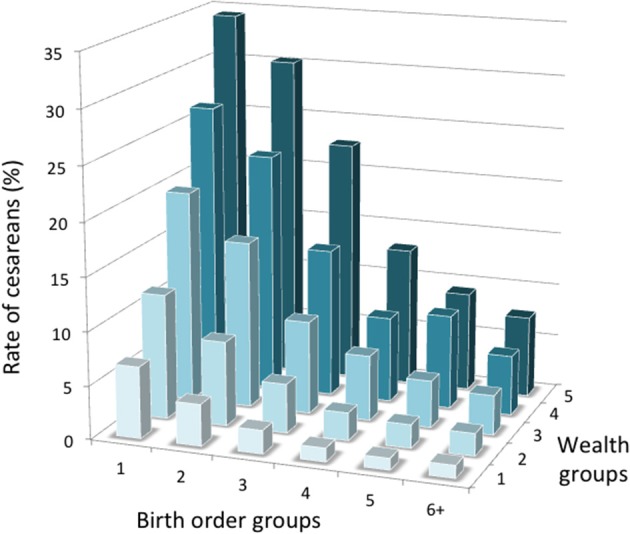
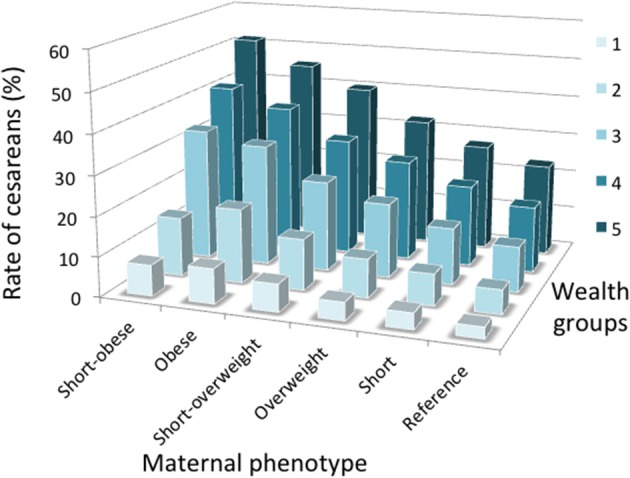
Background: Among contemporary human populations, rates of cesarean delivery vary substantially, making it difficult to know if the procedure is inadequately available, or used excessively relative to medical need. A much-cited evolutionary hypothesis attributed birth complications to an "obstetric dilemma," resulting from antagonistic selective pressures acting on maternal pelvic dimensions and fetal brain growth during hominin evolution. However, the childbirth challenges experienced by living humans may not be representative of those in the past, and may vary in association with trends in ecological conditions. We hypothesized that variability in maternal phenotype (height and nutritional status) may contribute to the risk of cesarean delivery. In many populations, high levels of child stunting contribute to a high frequency of short adult stature, while obesity is also becoming more common. The combination of short maternal stature and maternal overweight or obesity may substantially increase the risk of cesarean delivery. Methods: Using data from two large Indian health surveys from 2005-6 to 2015-2016, we tested associations of maternal somatic phenotype (short stature, overweight) with the risk of cesarean delivery, adjusting for confounding factors such as maternal age, birth order, rural/urban location, wealth and offspring sex. Results: Secular trends in maternal body mass index between surveys were greater than trends in height. Maternal short stature and overweight both increased the risk of cesarean delivery, most strongly when jointly present within individual women. These associations were independent of birth order, wealth, maternal age and rural/urban location. Secular trends in maternal phenotype explained 18% of the increase in cesarean rate over 10 years. Conclusion: Our results highlight how the emerging dual burden of malnutrition (persisting short adult stature which reflects persistent child stunting; increasing overweight in adults) is likely to impact childbirth in low and middle-income countries.
Keywords: India; South Asia; cesarean; dual burden of malnutrition; obesity; obstetric dilemma; overweight; short stature.
Figures


References
-
- Alkema L, Chou D, Hogan D, Zhang S, Moller AB, Gemmill A, et al. . Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet (2016) 387:462–74. 10.1016/S0140-6736(15)00838-7 - DOI - PMC - PubMed
-
- World Health Organization. Monitoring Emergency Obstetric Care: A Handbook. Geneva: World Health Organization; (2009).
LinkOut - more resources
Full Text Sources
Miscellaneous