

The impact of 2 years of high-intensity exercise training on a model of integrated cardiovascular regulation
- PMID: 30387144
- PMCID: PMC6332782
- DOI: 10.1113/JP276676
The impact of 2 years of high-intensity exercise training on a model of integrated cardiovascular regulation
Abstract
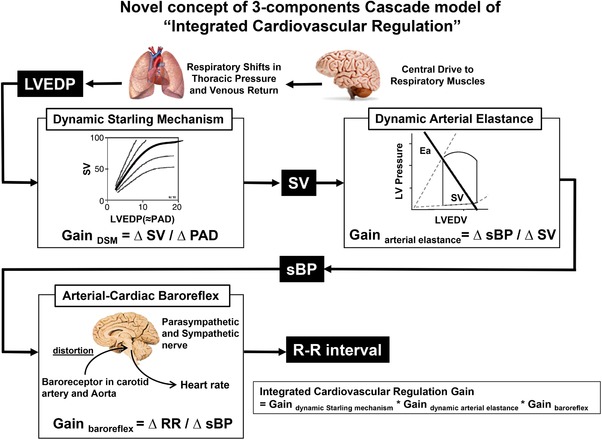
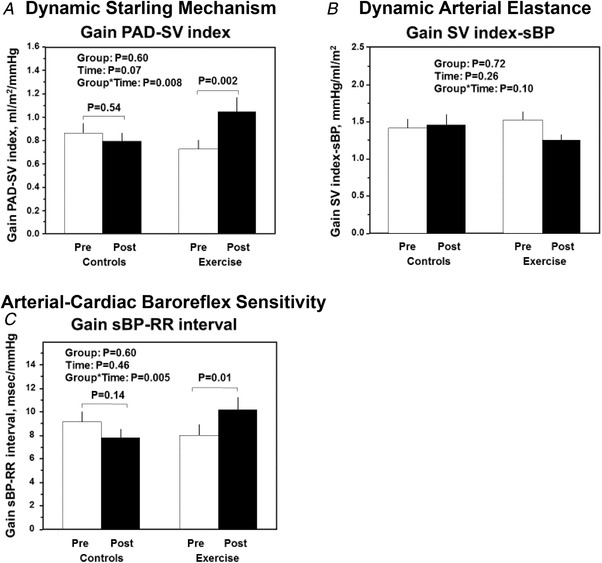
Key points: Heart rate variability, a common and easily measured index of cardiovascular dynamics, is the output variable of complicated cardiovascular and respiratory control systems. Both neural and non-neural control mechanisms may contribute to changes in heart rate variability. We previously developed an innovative method using transfer function analysis to assess the effect of prolonged exercise training on integrated cardiovascular regulation. In the present study, we modified and applied this to investigate the effect of 2 years of high-intensity training on circulatory components to tease out the primary effects of training. Our method incorporated the dynamic Starling mechanism, dynamic arterial elastance and arterial-cardiac baroreflex function. The dynamic Starling mechanism gain and arterial-cardiac baroreflex gain were significantly increased in the exercise group. These parameters remained unchanged in the controls. Conversely, neither group experienced a change in dynamic arterial elastance. The integrated cardiovascular regulation gain in the exercise group was 1.34-fold larger than that in the control group after the intervention. In these previously sedentary, otherwise healthy, middle-aged adults, 2 years of high-intensity exercise training improved integrated cardiovascular regulation by enhancing the dynamic Starling mechanism and arterial-cardiac baroreflex sensitivity.
Abstract: Assessing the effects of exercise training on cardiovascular variability is challenging because of the complexity of multiple mechanisms. In a prospective, parallel-group, randomized controlled study, we examined the effect of 2 years of high-intensity exercise training on integrated cardiovascular function, which incorporates the dynamic Starling mechanism, dynamic arterial elastance and arterial-cardiac baroreflex function. Sixty-one healthy participants (48% male, aged 53 years, range 52-54 years) were randomized to either 2 years of exercise training (exercise group: n = 34) or control/yoga group (controls: n = 27). Before and after 2 years, subjects underwent a 6 min recording of beat-by-beat pulmonary artery diastolic pressure (PAD), stroke volume index (SV index), systolic blood pressure (sBP) and RR interval measurements with controlled respiration at 0.2 Hz. The dynamic Starling mechanism, dynamic arterial elastance and arterial-cardiac baroreflex function were calculated by transfer function gain between PAD and SV index; SV index and sBP; and sBP and RR interval, respectively. Fifty-three participants (controls: n = 25; exercise group: n = 28) completed the intervention. After 2 years, the dynamic Starling mechanism gain (Group × Time interaction: P = 0.008) and the arterial-cardiac baroreflex gain (P = 0.005) were significantly increased in the exercise group but remained unchanged in the controls. There was no change in dynamic arterial elastance in either of the two groups. The integrated cardiovascular function gain in the exercise group increased 1.34-fold, whereas there was no change in the controls (P = 0.02). In these previously sedentary, otherwise healthy middle-aged adults, a 2 year programme of high-intensity exercise training improved integrated cardiovascular regulation by enhancing the dynamic Starling mechanism and arterial-cardiac baroreflex sensitivity, without changing dynamic arterial elastance.
Keywords: Arterial-Cardiac Baroreflex Sensitivity; Dynamic Arterial Elastance; Dynamic Starling mechanism; High Intensity Exercise Training; Integrative Cardiovascular Regulation; Ventricular-Arterial Coupling.
© 2018 The Authors. The Journal of Physiology © 2018 The Physiological Society.
Figures

Comment in
-
Mid-life crisis or mid-life gains: 2 years of high-intensity exercise is highly beneficial for the middle-aged heart.J Physiol. 2019 Apr;597(7):1787-1788. doi: 10.1113/JP277752. Epub 2019 Mar 10. J Physiol. 2019. PMID: 30730565 Free PMC article. No abstract available.
References
-
- Abdellatif M, Leite S, Alaa M, Oliveira‐Pinto J, Tavares‐Silva M, Fontoura D, Falcao‐Pires I, Leite‐Moreira AF & Lourenco AP (2016). Spectral transfer function analysis of respiratory hemodynamic fluctuations predicts end‐diastolic stiffness in preserved ejection fraction heart failure. Am J Physiol Heart Circ Physiol 310, H4–H13. - PubMed
-
- Chen C‐H, Fetics B, Nevo E, Rochitte CE, Chiou K‐R, Ding P‐A, Kawaguchi M & Kass DA (2001). Noninvasive single‐beat determination of left ventricular end‐systolic elastance in humans. J Am Coll Cardiol 38, 2028–2034. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical