

Non-invasive imaging of the coronary arteries
- PMID: 30388261
- PMCID: PMC6669405
- DOI: 10.1093/eurheartj/ehy670
Non-invasive imaging of the coronary arteries
Abstract
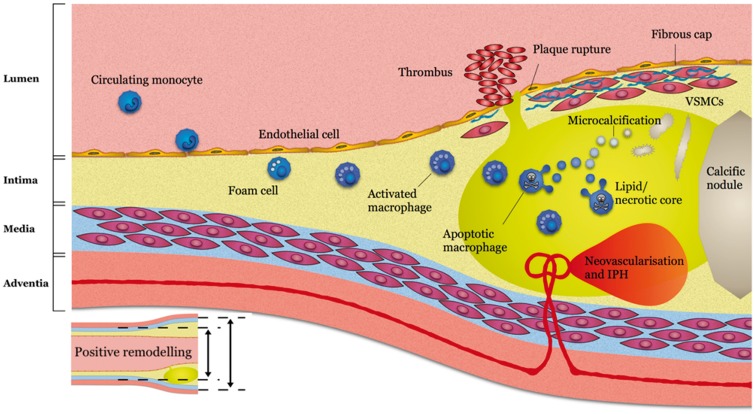
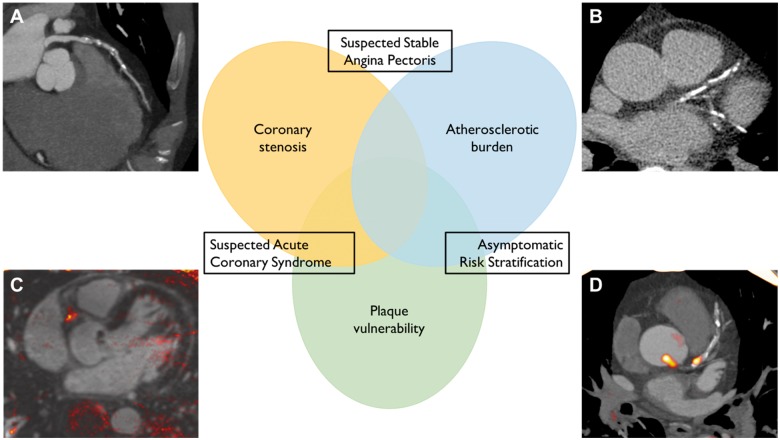
Non-invasive imaging of the coronary arteries is an enterprise in rapid development. From the research perspective, there is great demand for in vivo techniques that can reliably identify features of high-risk plaque that may offer insight into pathophysiological processes and act as surrogate indicators of response to therapeutic intervention. Meanwhile, there is clear clinical need for greater accuracy in diagnosis and prognostic stratification. Fortunately, ongoing technological improvements and emerging data from randomized clinical trials are helping make these elusive goals a reality. This review provides an update on the current status of non-invasive coronary imaging with computed tomography, magnetic resonance, and positron emission tomography with a focus on current clinical applications and future research directions.
Keywords: Computed tomography; Coronary heart disease; Magnetic resonance imaging; Positron emission tomography.
© The Author(s) 2018. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Townsend N, Wilson L, Bhatnagar P, Wickramasinghe K, Rayner M, Nichols M.. Cardiovascular disease in Europe: epidemiological update 2016. Eur Heart J 2016;37:3232–3245. - PubMed
-
- Adamson PD, Dweck MR, Newby DE.. The vulnerable atherosclerotic plaque: in vivo identification and potential therapeutic avenues. Heart 2015;101:1755–1766. - PubMed
-
- Rifkin RD, Parisi AF, Folland E.. Coronary calcification in the diagnosis of coronary artery disease. Am J Cardiol 1979;44:141–147. - PubMed
-
- Gerber TC, Carr JJ, Arai AE, Dixon RL, Ferrari VA, Gomes AS, Heller GV, McCollough CH, McNitt-Gray MF, Mettler FA, Mieres JH, Morin RL, Yester MV.. Ionizing radiation in cardiac imaging: a science advisory. Circulation 2009;119:1056–1065. - PubMed
