

Bronchiolitis obliterans syndrome-free survival after lung transplantation: An International Society for Heart and Lung Transplantation Thoracic Transplant Registry analysis
- PMID: 30391193
- PMCID: PMC6431291
- DOI: 10.1016/j.healun.2018.09.016
Bronchiolitis obliterans syndrome-free survival after lung transplantation: An International Society for Heart and Lung Transplantation Thoracic Transplant Registry analysis
Abstract
Background: Lung transplant (LTx) recipients have low long-term survival and a high incidence of bronchiolitis obliterans syndrome (BOS). However, few long-term, multicenter, and precise estimates of BOS-free survival (a composite outcome of death or BOS) incidence exist.
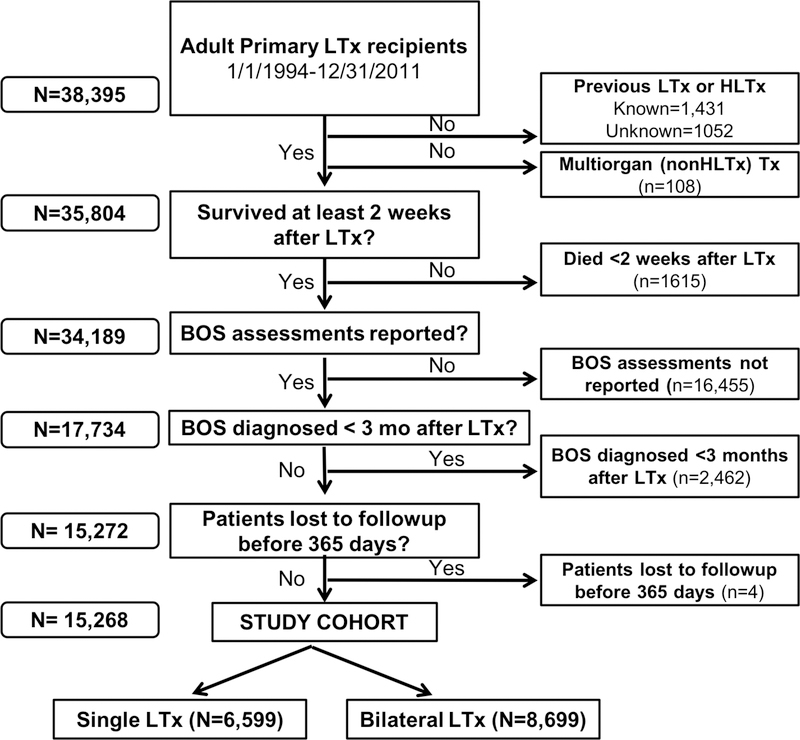
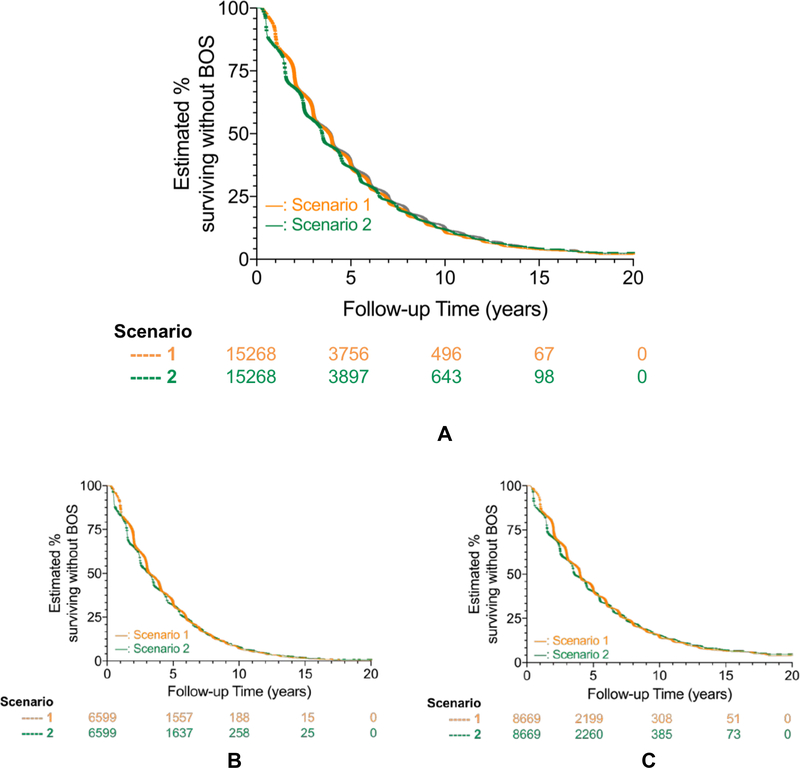
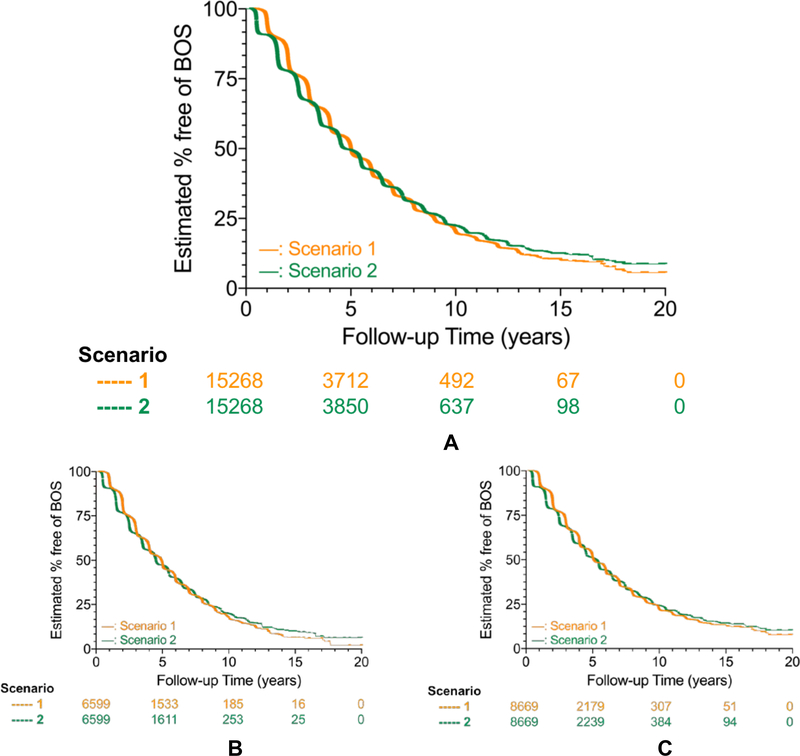
Methods: This retrospective cohort study of primary LTx recipients (1994-2011) reported to the International Society of Heart and Lung Transplantation Thoracic Transplant Registry assessed outcomes through 2012. For the composite primary outcome of BOS-free survival, we used Kaplan-Meier survival and Cox proportional hazards regression, censoring for loss to follow-up, end of study, and re-LTx. Although standard Thoracic Transplant Registry analyses censor at the last consecutive annual complete BOS status report, our analyses allowed for partially missing BOS data.
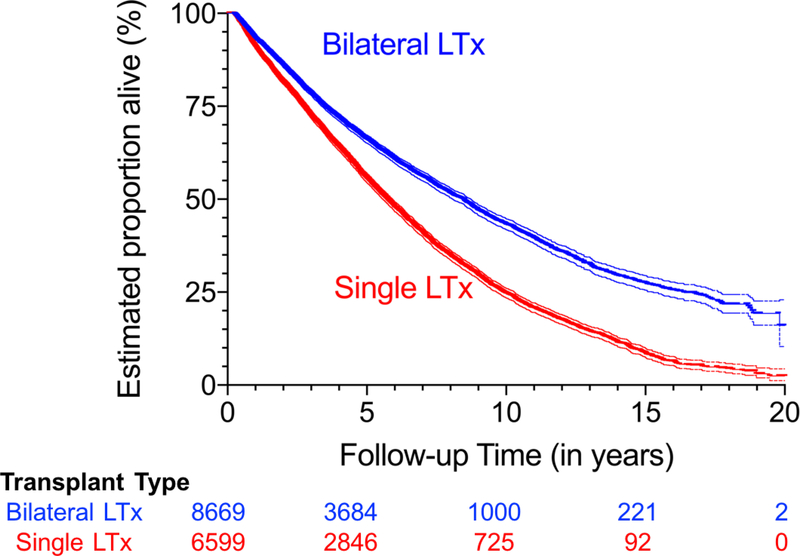
Results: Due to BOS reporting standards, 99.1% of the cohort received LTx in North America. During 79,896 person-years of follow-up, single LTx (6,599 of 15,268 [43%]) and bilateral LTx (8,699 of 15,268 [57%]) recipients had a median BOS-free survival of 3.16 years (95% confidence interval [CI], 2.99-3.30 years) and 3.58 years (95% CI, 3.53-3.72 years), respectively. Almost 90% of the single and bilateral LTx recipients developed the composite outcome within 10 years of transplantation. Standard Registry analyses "overestimated" median BOS-free survival by 0.42 years and "underestimated" the median survival after BOS by about a half-year for both single and bilateral LTx (p < 0.05).
Conclusions: Most LTx recipients die or develop BOS within 4 years, and very few remain alive and free from BOS at 10 years post-LTx. Less inclusive Thoracic Transplant Registry analytic methods tend to overestimate BOS-free survival. The Registry would benefit from improved international reporting of BOS and other chronic lung allograft dysfunction (CLAD) events.
Keywords: BOS-free survival; ISHLT Registry; bronchiolitis obliterans syndrome; chronic lung allograft dysfunction; lung transplant.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Freedom from chronic lung allograft dysfunction (CLAD) or CLAD-free survival: What's in a name?J Heart Lung Transplant. 2019 Jan;38(1):1-2. doi: 10.1016/j.healun.2018.11.005. Epub 2018 Nov 15. J Heart Lung Transplant. 2019. PMID: 30497817 No abstract available.
References
-
- Chambers DC, Yusen RD, Cherikh WS, et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-fourth Adult Lung And Heart-Lung Transplantation Report-2017; Focus Theme: Allograft ischemic time. J Heart Lung Transplant. 2017;36:1047–1059. - PubMed
-
- Verleden GM, Raghu G, Meyer KC, Glanville AR, Corris P. A new classification system for chronic lung allograft dysfunction. J Heart Lung Transplant. 2014;33:127–133. - PubMed
-
- Verleden GM, Vos R, Verleden SE, et al. Survival determinants in lung transplant patients with chronic allograft dysfunction. Transplantation. 2011;92:703–708. - PubMed
-
- Burke CM, Theodore J, Dawkins KD, et al. Post-transplant obliterative bronchiolitis and other late lung sequelae in human heart-lung transplantation. CHEST. 1984;86:824–829. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
