

Estimates of the Global Burden of Ambient , Ozone, and on Asthma Incidence and Emergency Room Visits
- PMID: 30392403
- PMCID: PMC6371661
- DOI: 10.1289/EHP3766
Estimates of the Global Burden of Ambient , Ozone, and on Asthma Incidence and Emergency Room Visits
Abstract
Background: Asthma is the most prevalent chronic respiratory disease worldwide, affecting 358 million people in 2015. Ambient air pollution exacerbates asthma among populations around the world and may also contribute to new-onset asthma.
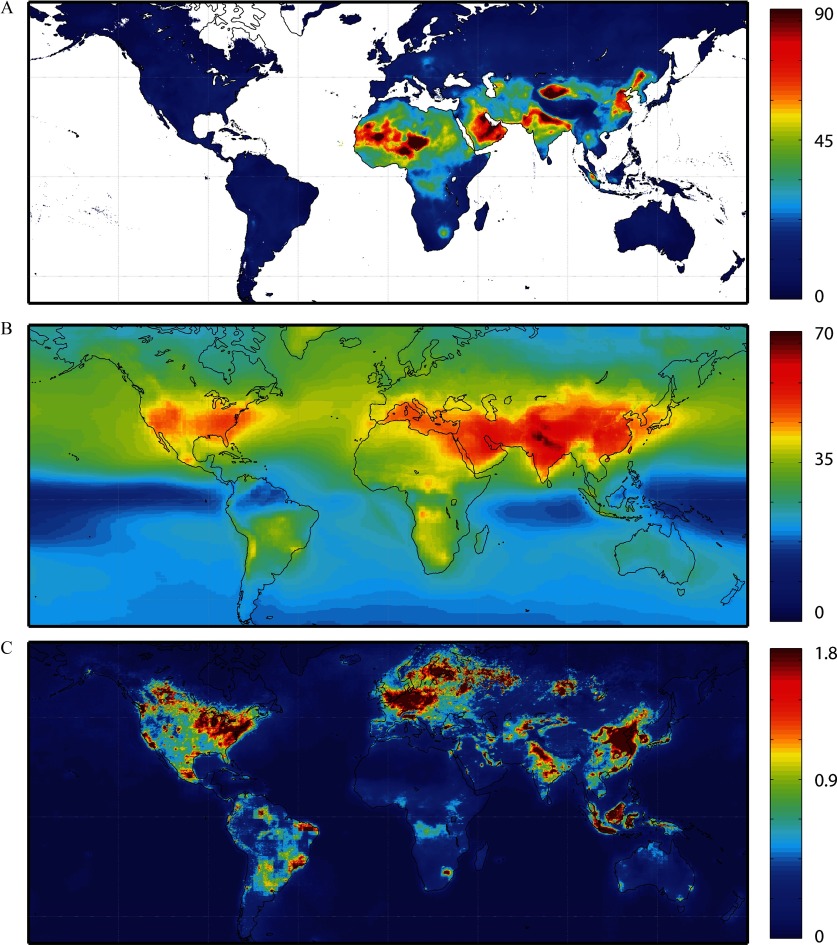
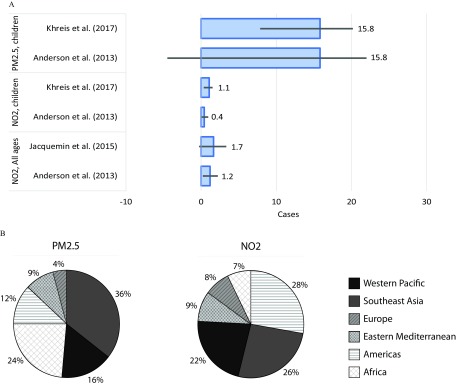
Objectives: We aimed to estimate the number of asthma emergency room visits and new onset asthma cases globally attributable to fine particulate matter (), ozone, and nitrogen dioxide () concentrations.
Methods: We used epidemiological health impact functions combined with data describing population, baseline asthma incidence and prevalence, and pollutant concentrations. We constructed a new dataset of national and regional emergency room visit rates among people with asthma using published survey data.
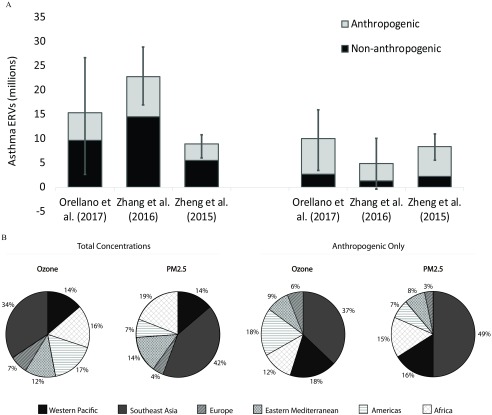
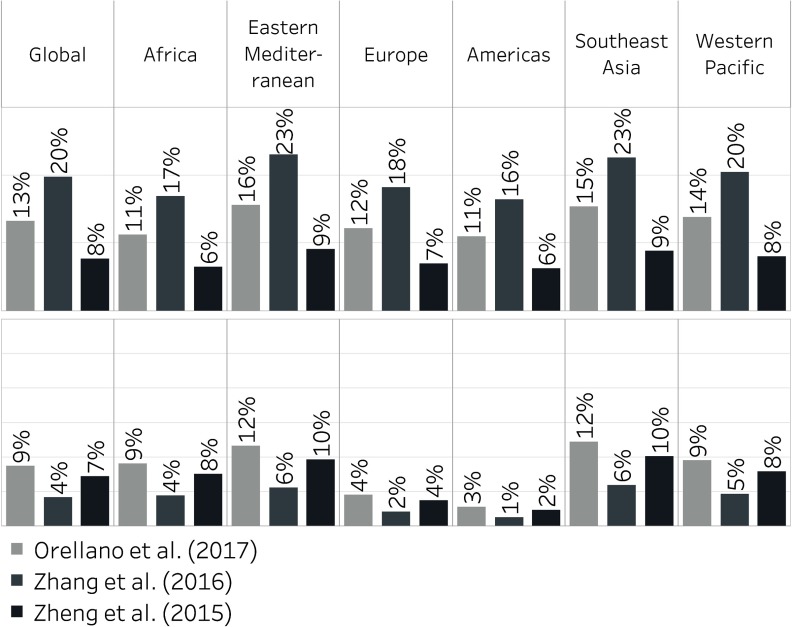
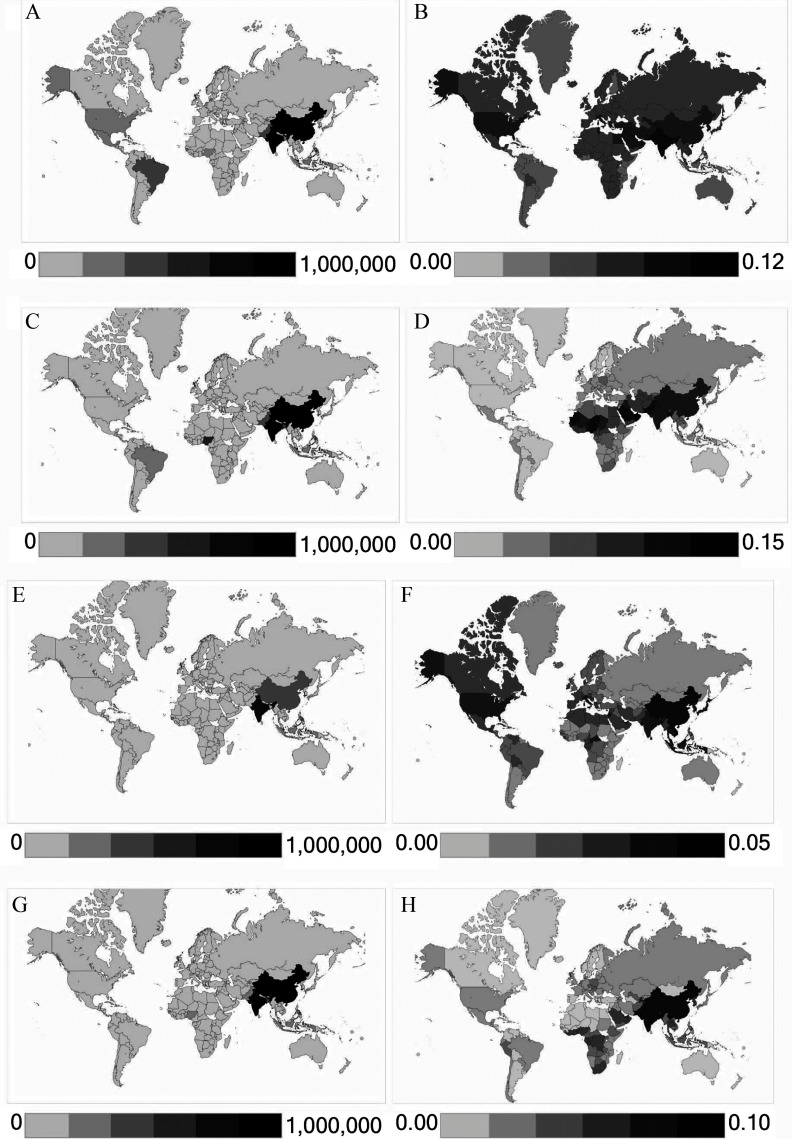
Results: We estimated that 9–23 million and 5–10 million annual asthma emergency room visits globally in 2015 could be attributable to ozone and , respectively, representing 8–20% and 4–9% of the annual number of global visits, respectively. The range reflects the application of central risk estimates from different epidemiological meta-analyses. Anthropogenic emissions were responsible for and 73% of ozone and impacts, respectively. Remaining impacts were attributable to naturally occurring ozone precursor emissions (e.g., from vegetation, lightning) and (e.g., dust, sea salt), though several of these sources are also influenced by humans. The largest impacts were estimated in China and India.
Conclusions: These findings estimate the magnitude of the global asthma burden that could be avoided by reducing ambient air pollution. We also identified key uncertainties and data limitations to be addressed to enable refined estimation. https://doi.org/10.1289/EHP3766.
Figures
Comment in
-
Asthma Actors: Estimating How Much Specific Air Pollutants Contribute to ER Visits.Environ Health Perspect. 2019 Jul;127(7):74001. doi: 10.1289/EHP4799. Epub 2019 Jul 17. Environ Health Perspect. 2019. PMID: 31313937 Free PMC article. No abstract available.
References
-
- Anderson HR, Favarato G, Atkinson RW. 2013. Long-term exposure to air pollution and the incidence of asthma: meta-analysis of cohort studies. Air Qual Atmos Health 6(1):47–56, 10.1007/s11869-011-0144-5. - DOI