

Pulmonary artery embolism by a metal fragment after a booby trap explosion in a combat patient injured in the armed conflict in East Ukraine: a case report and review of the literature
- PMID: 30392466
- PMCID: PMC6217764
- DOI: 10.1186/s13256-018-1834-5
Pulmonary artery embolism by a metal fragment after a booby trap explosion in a combat patient injured in the armed conflict in East Ukraine: a case report and review of the literature
Abstract
Background: Pulmonary artery embolization due to projectile embolus is a rare complication in combat patients. Such embolization is rare for combat patients in the ongoing armed conflict, in East Ukraine since 2014.
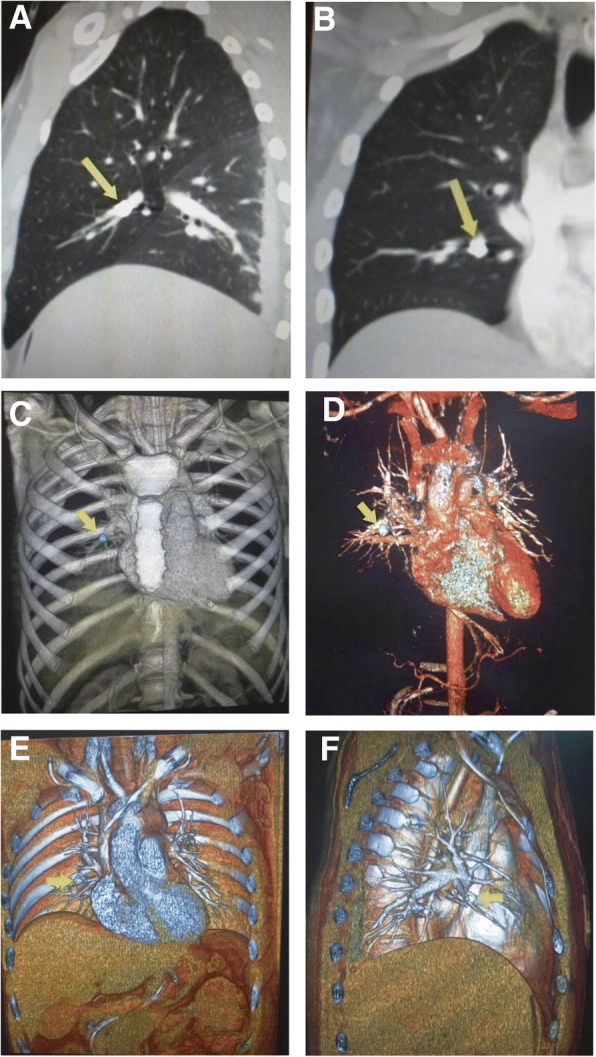
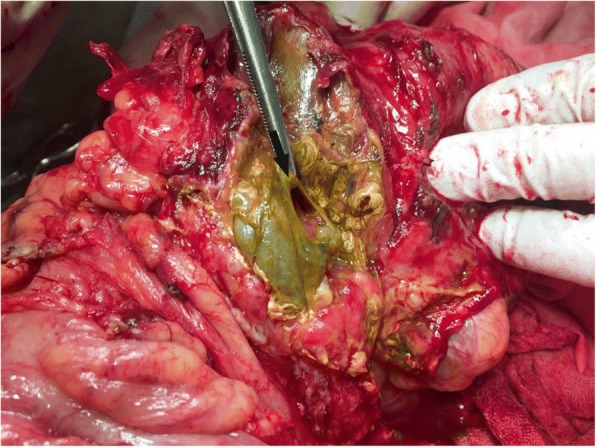
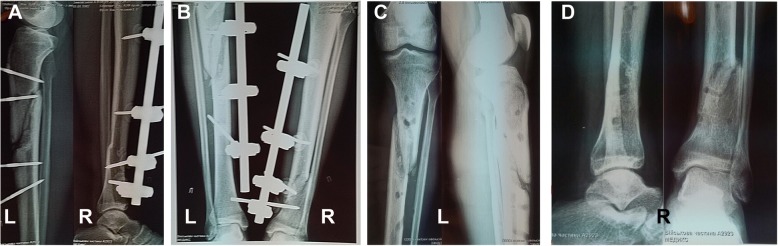
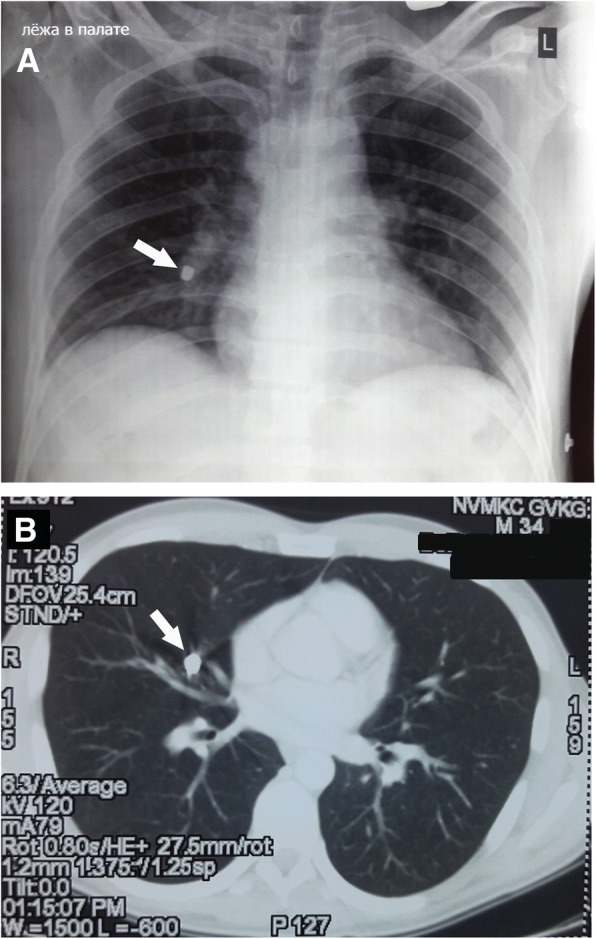
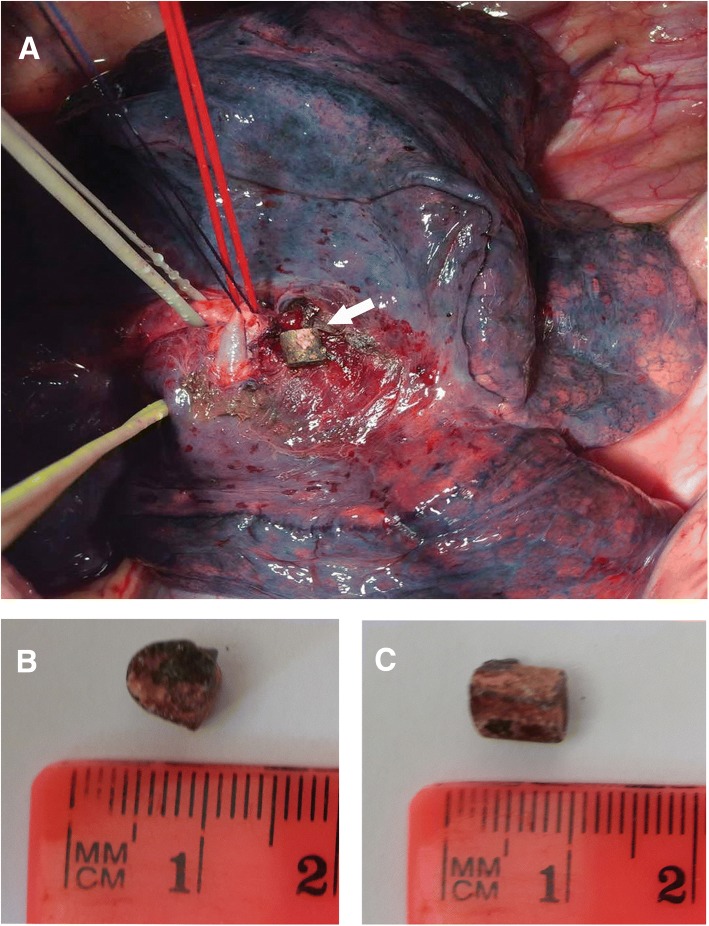
Case presentation: We report a clinical case of a 34-year-old Caucasian combat patient who was injured after an explosion of a booby trap hand grenade. This soldier was diagnosed with severe abdominal and skeletal trauma: damage of the duodenum and transverse colon, internal bleeding due to inferior vena cava damage and fractures of both lower extremities. The patient was treated at a highly specialized surgical center within the "golden hour" time. Whole-body computed tomography scan was performed as a routine screening method for hemodynamically stable patients, at which we identified a projectile embolus due to the explosion of a booby trap hand grenade in the right midlobar pulmonary artery. Our patient had no clinical manifestation of pulmonary artery embolism. At follow-up, our patient was diagnosed with the following complications: multiple necrosis and perforations of the transverse colon leading to a fecal peritonitis; duodenum suture line leakage caused the formation of a duodenal fistula; postoperative wound infection. These complications required multiple secondary operations, and in accordance to the principles of damage-control tactics, the extraction of projectile-embolus was postponed. Open surgery retrieval of the metal fragment was successfully performed on the 80th day after injury. Our patient was discharged from the hospital on day 168th after injury.
Conclusions: Literature analysis shows a significant difference of clinical management for patient with projectile embolism in hybrid war settings as compared to previously described cases of combat and civil gunshot injuries. Damage control tactics and the concept of the "golden hour" are highly effective for those injured in a hybrid war. A whole-body computed tomography scan is an effective screening method for asymptomatic patients with projectile-embolism of the great vessels. The investigation of a greater cohort of combat patients with severe injuries and projectile-embolism should be performed in order to develop a better guideline for these patients and to save more lives.
Keywords: Armed conflict in Ukraine; Combat trauma; Damage control; Hybrid warfare; Projectile-embolus.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by ethical committee at Bogomolets National Medical University (07/10/2015 Nr.90).
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Retrieval of ferromagnetic fragments from the lung using video-assisted thoracoscopic surgery and magnetic tool: a case report of combat patient injured in the war in Ukraine.Int J Emerg Med. 2023 Aug 24;16(1):51. doi: 10.1186/s12245-023-00527-8. Int J Emerg Med. 2023. PMID: 37620806 Free PMC article.
-
Management of gunshot injury to the abdominal aorta and inferior vena cava: a case report of a combat patient wounded in the Russo-Ukrainian war.Int J Emerg Med. 2024 Sep 5;17(1):113. doi: 10.1186/s12245-024-00690-6. Int J Emerg Med. 2024. PMID: 39237874 Free PMC article.
-
Pulmonary Artery Bullet Embolism following Cardiac Gunshot Wound.Ann Vasc Surg. 2016 Oct;36:290.e11-290.e14. doi: 10.1016/j.avsg.2016.02.038. Epub 2016 Jul 6. Ann Vasc Surg. 2016. PMID: 27395810
-
Endovascular Removal of Pulmonary Artery Bullet Embolus: Case Report and Literature Review.Vasc Endovascular Surg. 2024 Oct;58(7):789-797. doi: 10.1177/15385744241264791. Epub 2024 Jul 21. Vasc Endovascular Surg. 2024. PMID: 39033397 Review.
-
Bullet embolism.J Cardiovasc Surg (Torino). 1989 Jul-Aug;30(4):584-90. J Cardiovasc Surg (Torino). 1989. PMID: 2674155 Review.
Cited by
-
Retained bullet in the neck after gunshot wounds to the chest and arm in combat patient injured in the war in Ukraine: A case report.Int J Surg Case Rep. 2022 Oct;99:107658. doi: 10.1016/j.ijscr.2022.107658. Epub 2022 Sep 14. Int J Surg Case Rep. 2022. PMID: 36116307 Free PMC article.
-
Craniocerebral gunshot injury bullet migration to the cardiac right ventricle.Surg Neurol Int. 2021 Sep 30;12:491. doi: 10.25259/SNI_221_2021. eCollection 2021. Surg Neurol Int. 2021. PMID: 34754541 Free PMC article.
-
Management of thoracoabdominal gunshot injuries by using minimally invasive surgery at role 2 deployed field hospitals in Ukraine.BMC Surg. 2024 Jun 14;24(1):183. doi: 10.1186/s12893-024-02475-3. BMC Surg. 2024. PMID: 38877409 Free PMC article.
References
-
- Khomenko I, Shapovalov V, Tsema I, Makarov G, Palytsia R, Zavodovskyi I, et al. Hydrodynamic rupture of liver in combat patient: a case of successful application of “damage control” tactic in area of the hybrid war in East Ukraine. Surg Case Rep. 2017;3(1):88. doi: 10.1186/s40792-017-0363-6. - DOI - PMC - PubMed
-
- Rácz A. Russia’s hybrid war in Ukraine : breaking the enemy’s ability to resist. Helsinki: Ulkopoliittinen Instituutti; 2015. p. 99.
-
- Banasik Mirosław. How to understand the hybrid war. Securitologia. 2015;21(1):19–34. doi: 10.5604/18984509.1184214. - DOI
-
- Tsema IV, Bespalenko AA, Dinets AV, Koval BM, Mishalov VG. Study of damaging factors of contemporary war, leading to the limb loss. Novosti Khirurgii. 2018;26(3):321–331. doi: 10.18484/2305-0047.2018.3.321. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
