

Dose-response relationship between docosahexaenoic acid (DHA) intake and lower rates of early preterm birth, low birth weight and very low birth weight
- PMID: 30392575
- PMCID: PMC9837789
- DOI: 10.1016/j.plefa.2018.09.002
Dose-response relationship between docosahexaenoic acid (DHA) intake and lower rates of early preterm birth, low birth weight and very low birth weight
Abstract
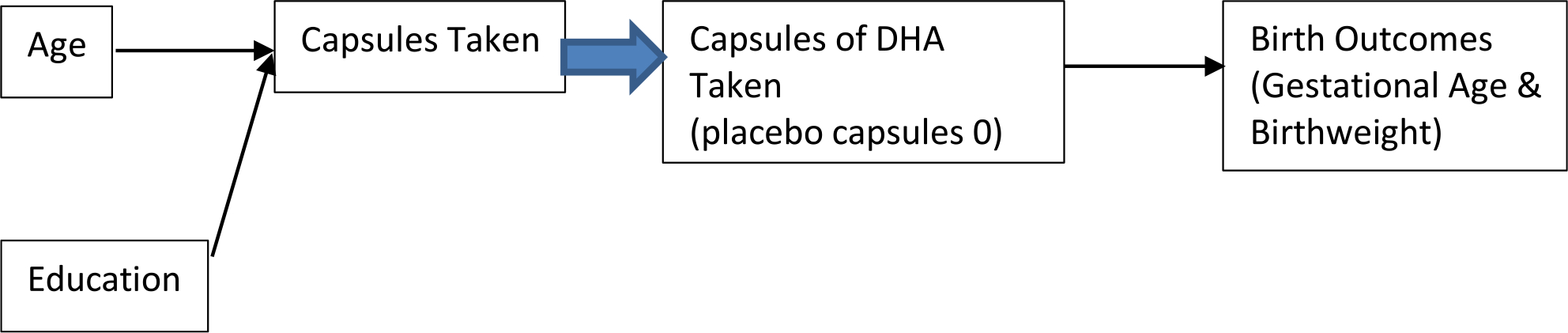
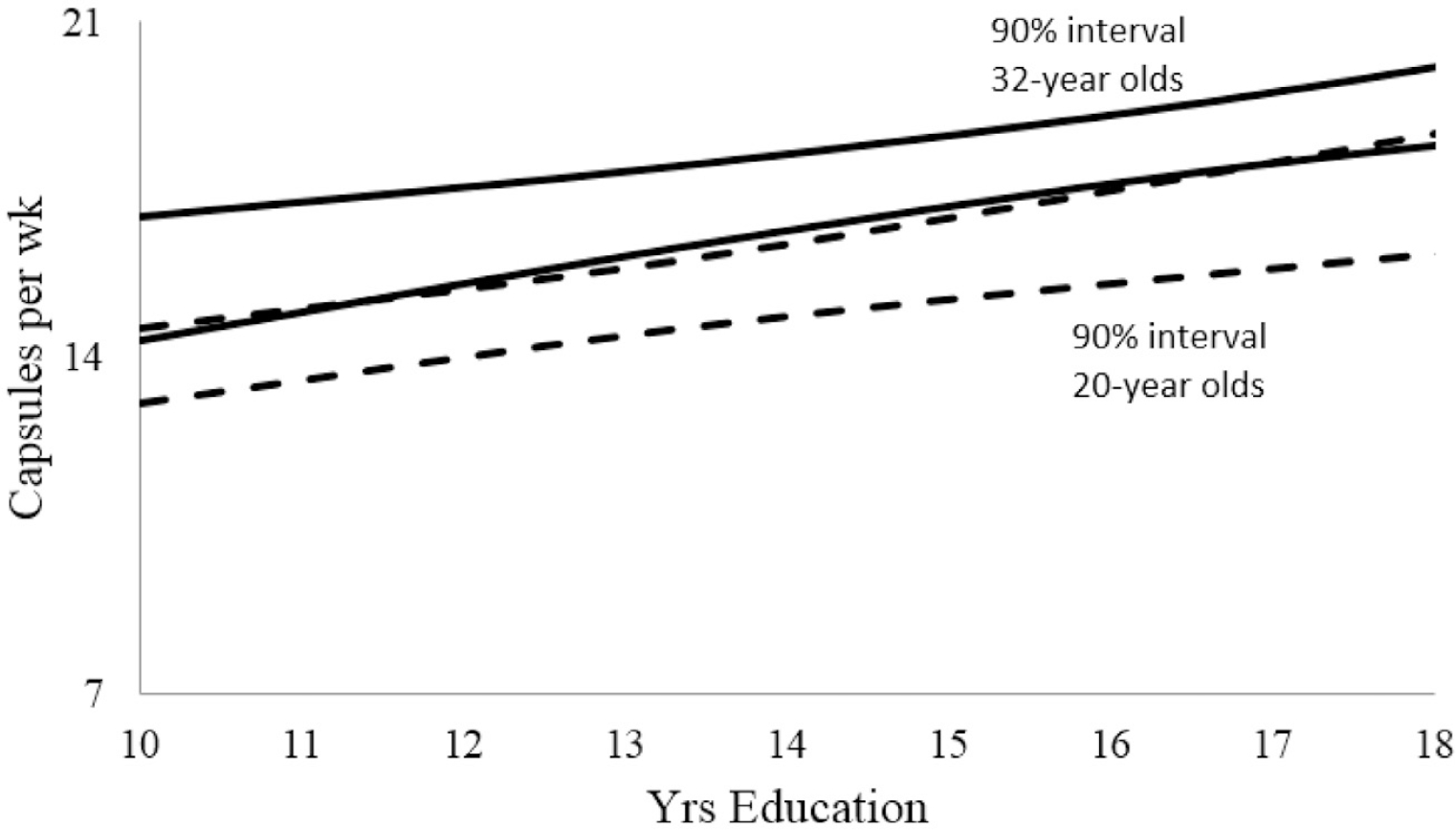
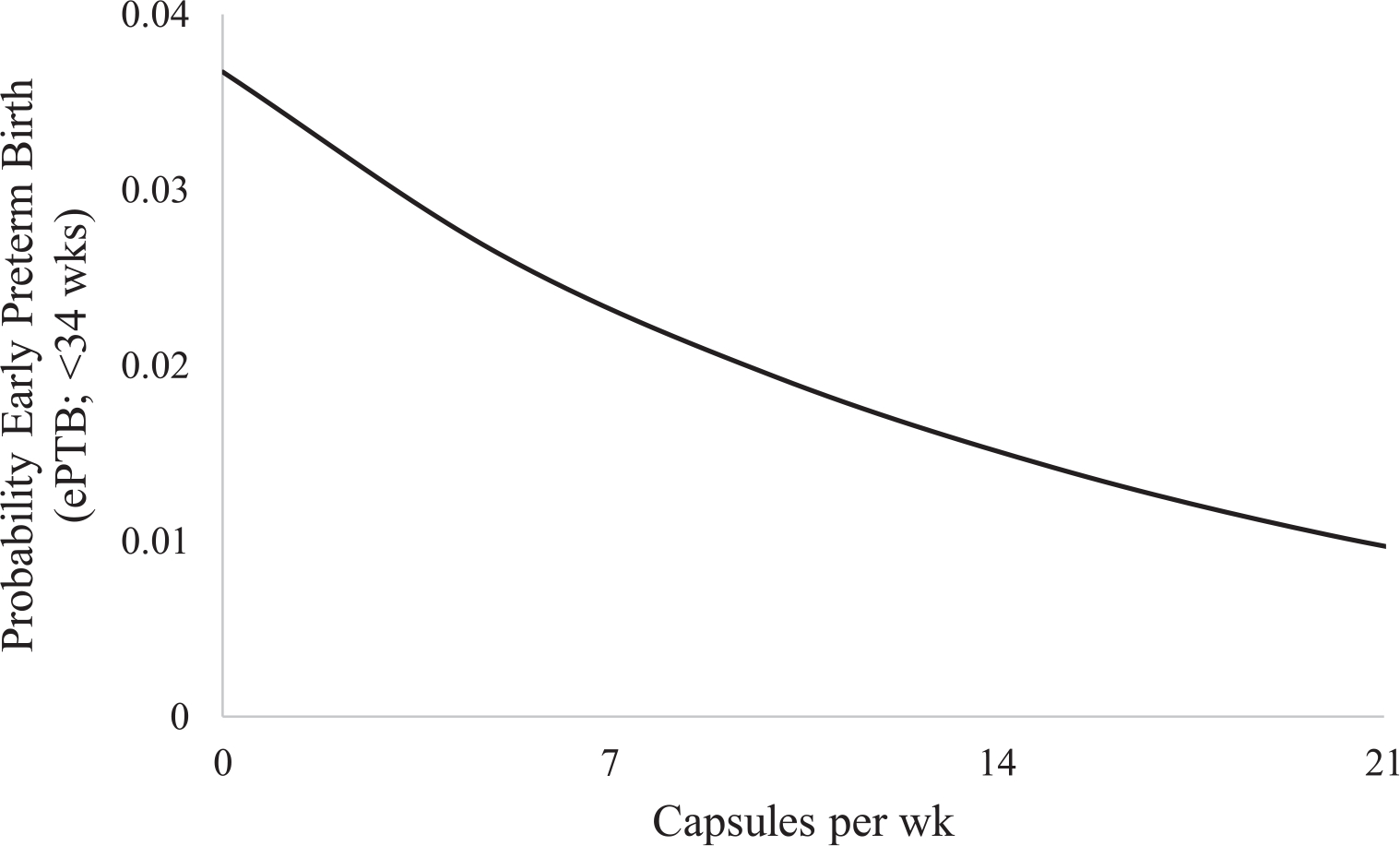
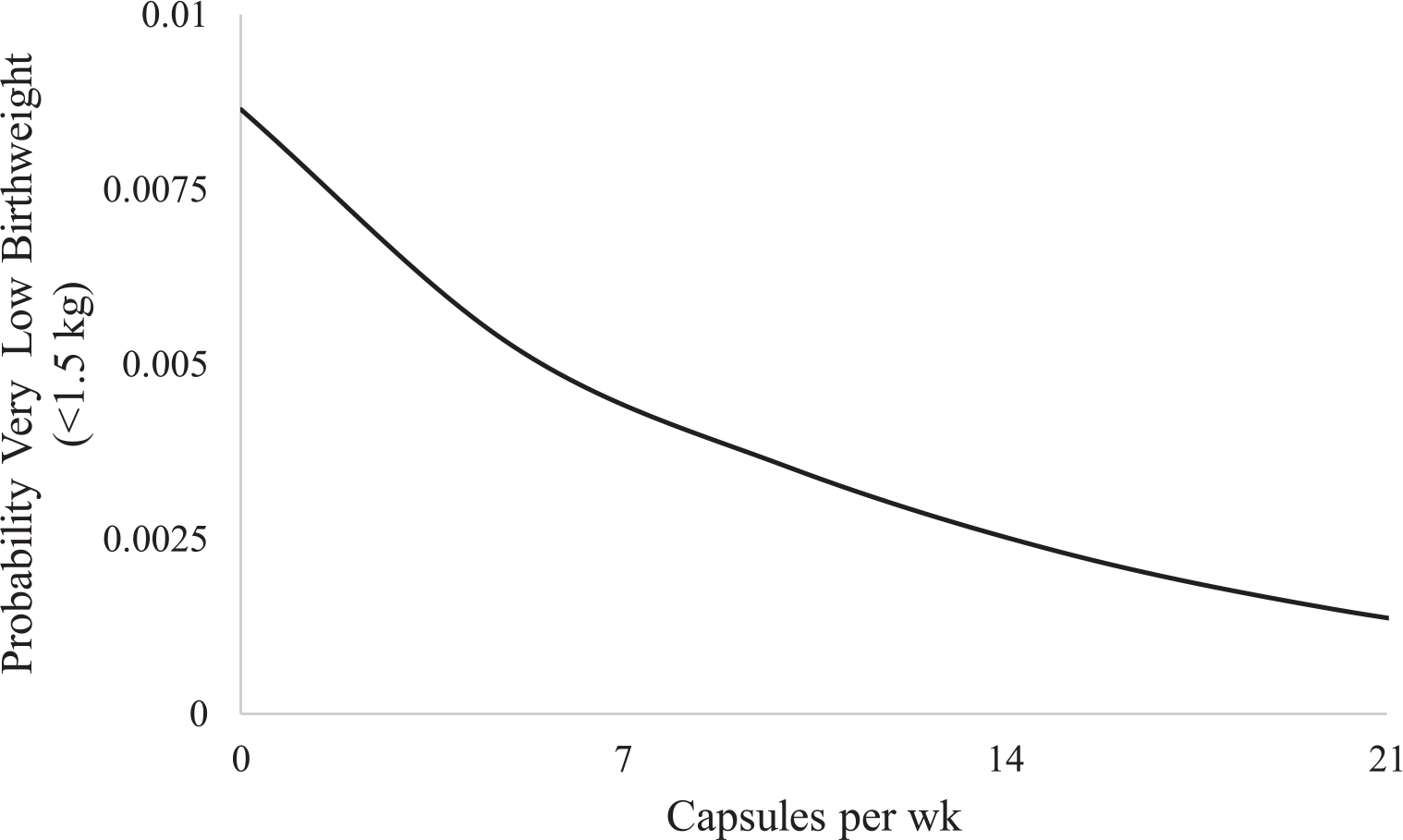
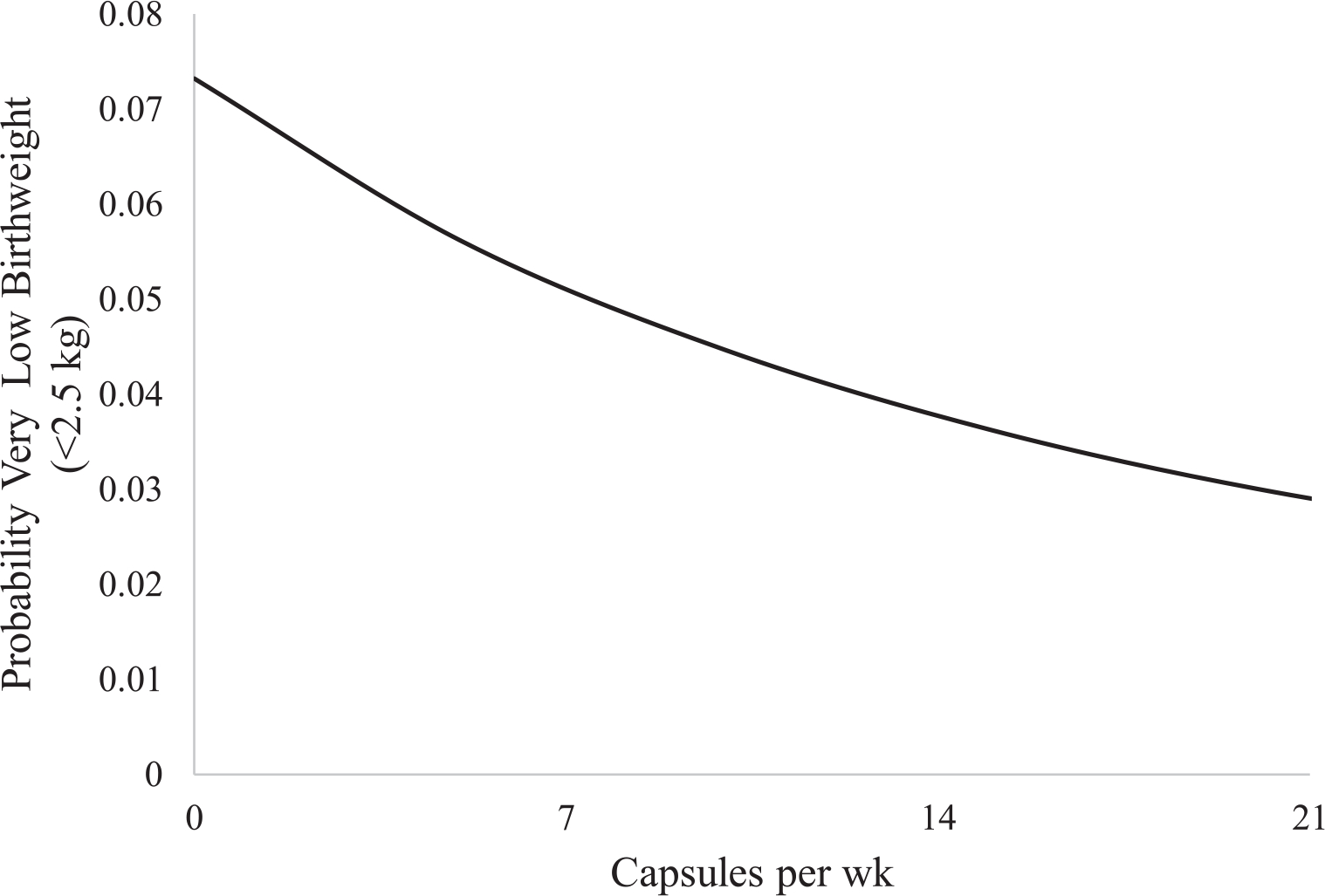
As previously reported, intention-to-treat findings from our phase III randomized clinical trial found that a supplement of 600 mg docosahexaenoic acid (DHA)/day during the last half of pregnancy reduced the incidence of early preterm birth (ePTB, <34 weeks gestation) and very low birth weight (VLBW < 1500 g) offspring. Given the potentially immense clinical significance of these findings, the goal of this secondary analysis was to (1) identify maternal characteristics related with capsule intake (i.e. DHA dose exposure) and (2) determine if DHA dose was associated with low (<2500 g) and very low birth weight after controlling for any relevant maternal characteristics. Three hundred forty-five pregnant mothers were recruited from hospitals in the Kansas City metropolitan area between 2006 and 2011. Most participants (n = 299) were from the phase III trial mentioned above, but we also included 46 participants from a second smaller, randomized trial that utilized an identical intervention design and was conducted concurrent to the larger trial. Both trials assigned participants to either 3 daily capsules of vegetable oil without DHA (n = 169) or 3 daily capsules of 200 mg DHA each (n = 176). Total capsules consumed was recorded by pharmacy supervised capsule count or participant self-report when needed. Maternal age, education, race and gestational age at delivery as well as infant birth weight were available for both trials. A Bayesian linear model indicated capsule intake increased with maternal age (p = 0.0100) and years of education (p = 0.0002). A Bayesian bivariate mixture-model associated capsule intake with simultaneous lower probability of ePTB, low birth weight (LBW, <2500 g) and VLBW (p = 0.0327). This, in conjunction with the positive findings in the clinical trial, support the need for future research to examine intervention methods to improve capsule compliance strategies in younger and less educated mothers.
Trial registration: ClinicalTrials.gov NCT00266825.
Keywords: Birth weight; Compliance; Docosahexaenoic acid; Placebo; Preterm birth.
Copyright © 2018. Published by Elsevier Ltd.
Figures
References
-
- Kar S, Wong M, Rogozinska E, Thangaratinam S, Effects of omega-3 fatty acids in prevention of early preterm delivery: a systematic review and meta-analysis of randomized studies, Eur. J. Obstet. Gynecol. Reprod. Biol. 198 (2016) 40–46. - PubMed
-
- Makrides M, Gibson RA, McPhee AJ, Yelland L, Quinlivan J, Ryan P, Effect of DHA supplementation during pregnancy on maternal depression and neurodevelopment of young children: a randomized controlled trial, JAMA 304 (2010) 1675–1683. - PubMed
-
- Ramakrishnan U, Stein AD, Parra-Cabrera S, Wang M, Imhoff-Kunsch B, Juarez-Marquez S, Rivera J, Martorell R, Effects of docosahexaenoic acid supplementation during pregnancy on gestational age and size at birth: randomized, double-blind, placebo-controlled trial in Mexico, Food Nutr. Bull. 31 (2010) S108–S116. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
