

ICU Admission Muscle and Fat Mass, Survival, and Disability at Discharge: A Prospective Cohort Study
- PMID: 30392790
- PMCID: PMC6363817
- DOI: 10.1016/j.chest.2018.10.023
ICU Admission Muscle and Fat Mass, Survival, and Disability at Discharge: A Prospective Cohort Study
Abstract
Background: Skeletal muscle dysfunction occurring as a result of ICU admission associates with higher mortality. Although preadmission higher BMI correlates with better outcomes, the impact of baseline muscle and fat mass has not been defined. We therefore investigated the association of skeletal muscle and fat mass at ICU admission with survival and disability at hospital discharge.
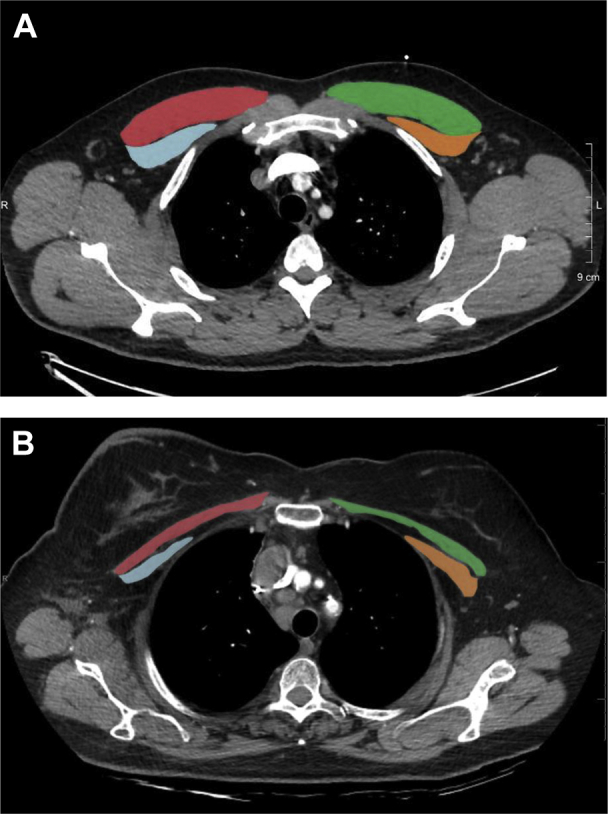
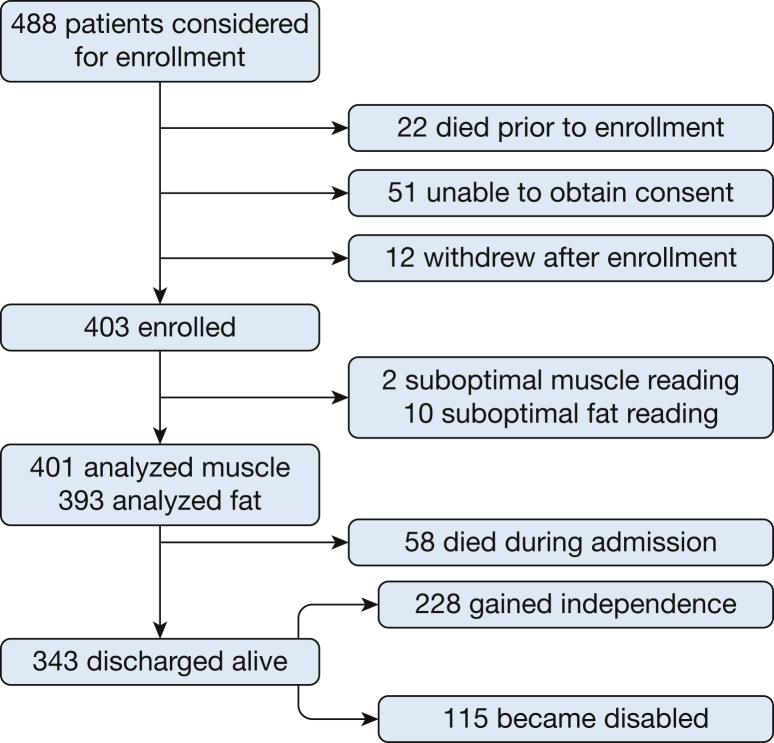
Methods: This single-center, prospective, observational cohort study included medical ICU (MICU) patients from an academic institution in the Unites States. A total of 401 patients were evaluated with pectoralis muscle area (PMA) and subcutaneous adipose tissue (SAT) determinations conducted by CT scanning at the time of ICU admission, which were later correlated with clinical outcomes accounting for potential confounders.
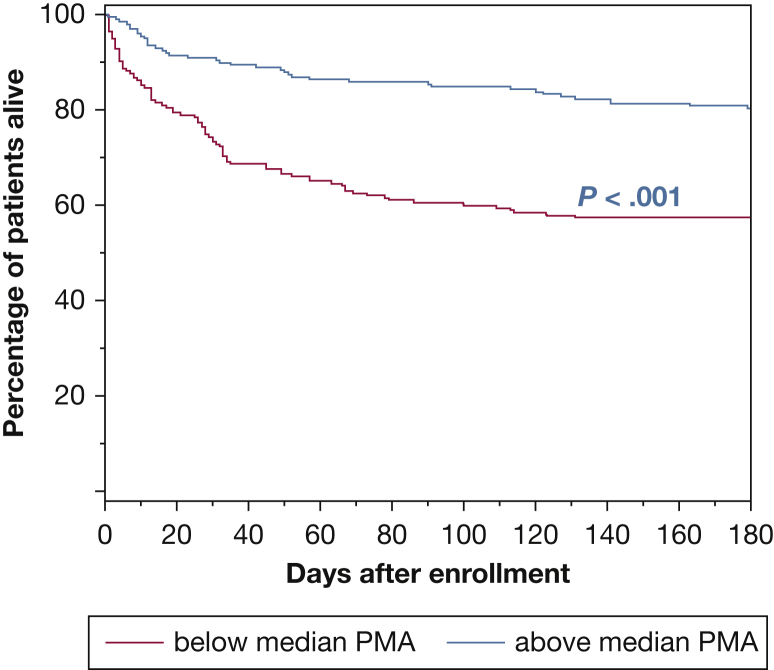
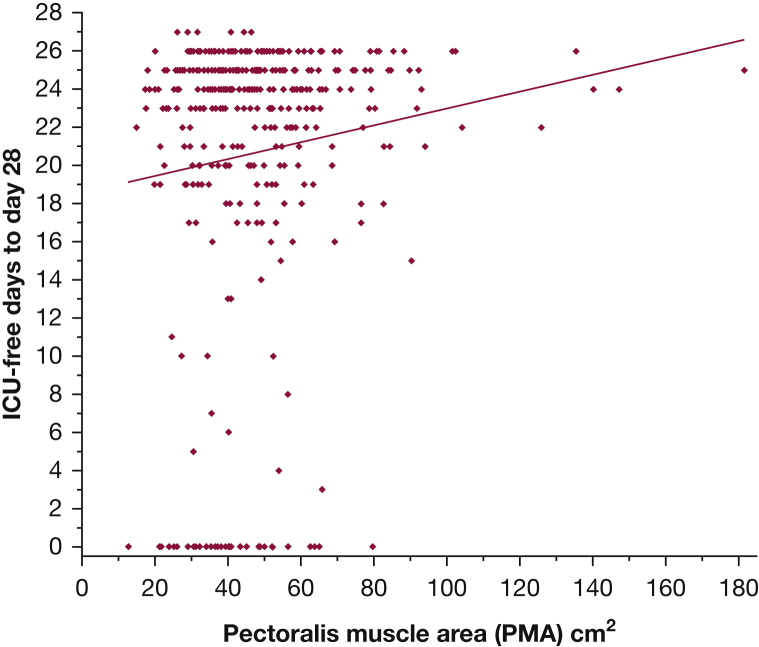
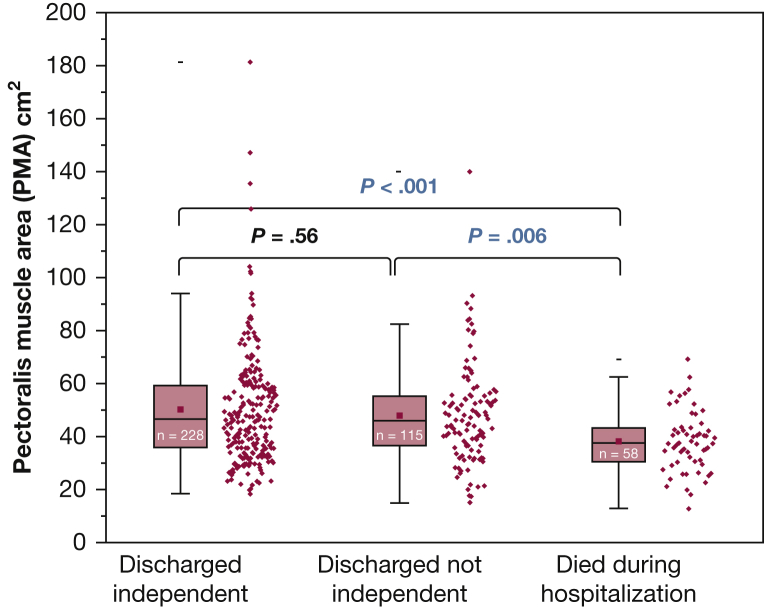
Results: Larger admission PMA was associated with better outcomes, including higher 6-month survival (OR, 1.03; 95% CI, 1.01-1.04; P < .001), lower hospital mortality (OR, 0.96; 95% CI, 0.93-0.98; P < .001), and more ICU-free days (slope, 0.044 ± 0.019; P = .021). SAT was not significantly associated with any of the measured outcomes. In multivariable analyses, PMA association persisted with 6 months and hospital survival and ICU-free days, whereas SAT remained unassociated with survival or other outcomes. PMA was not associated with regaining of independence at the time of hospital discharge (OR, 0.99; 95% CI, 0.98-1.01; P = .56).
Conclusions: In this study cohort, ICU admission PMA was associated with survival during and following critical illness; it was unable to predict regaining an independent lifestyle following discharge. ICU admission SAT mass was not associated with survival or other measured outcomes.
Keywords: adipose tissue; critical illness; frailty; muscle wasting; pectoralis muscle area.
Published by Elsevier Inc.
Figures
References
-
- Puthucheary Z.A. Acute skeletal muscle wasting in critical illness. JAMA. 2013;310:1591–1600. - PubMed
-
- Ali N.A. Acquired weakness, handgrip strength, and mortality in critically ill patients. Am J Respir Crit Care Med. 2008;178:261–268. - PubMed
-
- Sharshar T. Presence and severity of intensive care unit-acquired paresis at time of awakening are associated with increased intensive care unit and hospital mortality. Crit Care Med. 2009;37:3047–3053. - PubMed
-
- De Jonghe B. Respiratory weakness is associated with limb weakness and delayed weaning in critical illness. Crit Care Med. 2007;35:2007–2015. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
