

Storage diseases with hypertrophic cardiomyopathy phenotype
- PMID: 30393640
- PMCID: PMC6209457
- DOI: 10.21542/gcsp.2018.28
Storage diseases with hypertrophic cardiomyopathy phenotype
Abstract
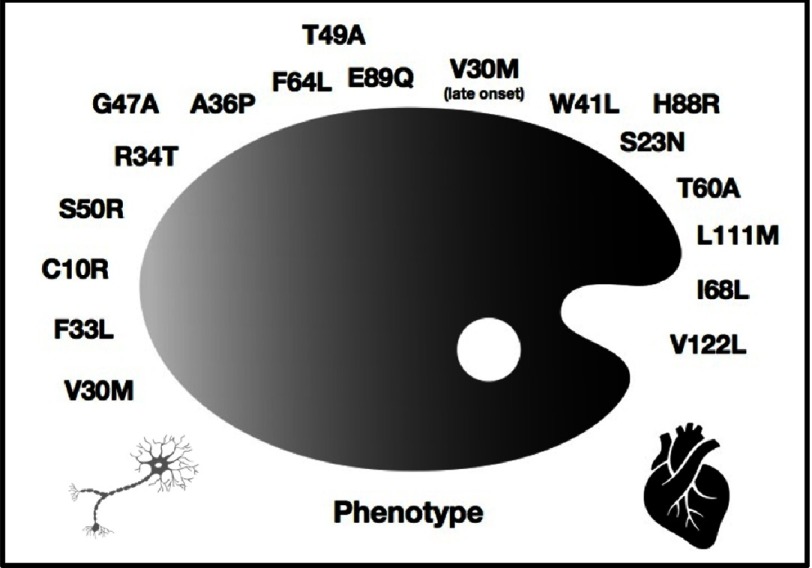
Never judge a book by its cover, nor assume hypertrophic cardiomyopathy (HCM) as sarcomeric, as appearances can deceive. HCM phenocopies account for a 5-10% of the cases, mainly represented by storage diseases, flagged by the increasing prevalence of senile cardiac amyloid in developing countries. Multisystemic and heterogeneous presentation of these entities is a challenge for clinicians, and time delay in diagnosis is a major concern. Promising drugs and gene-specific tailored therapies are under development, therefore, more than ever, appropriate understanding of these conditions is mandatory for adequate early treatment and counselling. In this review, storage disorders will be classified as extracellular and intracellular deposit storage diseases, focusing our attention on the most prevalent conditions from the cardiologist's perspective.
Figures


Similar articles
-
Beyond Sarcomeric Hypertrophic Cardiomyopathy: How to Diagnose and Manage Phenocopies.Curr Cardiol Rep. 2022 Nov;24(11):1567-1585. doi: 10.1007/s11886-022-01778-2. Epub 2022 Sep 2. Curr Cardiol Rep. 2022. PMID: 36053410 Review.
-
Mimics of Hypertrophic Cardiomyopathy - Diagnostic Clues to Aid Early Identification of Phenocopies.Arrhythm Electrophysiol Rev. 2013 Apr;2(1):36-40. doi: 10.15420/aer.2013.2.1.36. Arrhythm Electrophysiol Rev. 2013. PMID: 26835038 Free PMC article.
-
Diagnostic Clues for the Diagnosis of Nonsarcomeric Hypertrophic Cardiomyopathy (Phenocopies): Amyloidosis, Fabry Disease, and Mitochondrial Disease.J Cardiovasc Echogr. 2018 Apr-Jun;28(2):120-123. doi: 10.4103/jcecho.jcecho_2_18. J Cardiovasc Echogr. 2018. PMID: 29911009 Free PMC article.
-
MR Imaging in Hypertrophic Cardiomyopathy: From Magnet to Bedside.Radiology. 2014 Nov;273(2):329-48. doi: 10.1148/radiol.14131626. Radiology. 2014. PMID: 25340269 Review.
-
Relationship between aetiology and left ventricular systolic dysfunction in hypertrophic cardiomyopathy.Heart. 2017 Feb 15;103(4):300-306. doi: 10.1136/heartjnl-2016-310138. Epub 2016 Oct 24. Heart. 2017. PMID: 27798053
Cited by
-
Retrospective evaluation of hypertrophic cardiomyopathy in 68 dogs.J Vet Intern Med. 2022 May;36(3):865-876. doi: 10.1111/jvim.16402. Epub 2022 Mar 24. J Vet Intern Med. 2022. PMID: 35322461 Free PMC article.
-
Spns1-dependent endocardial lysosomal function drives valve morphogenesis through Notch1-signaling.iScience. 2024 Nov 19;27(12):111406. doi: 10.1016/j.isci.2024.111406. eCollection 2024 Dec 20. iScience. 2024. PMID: 39720516 Free PMC article.
-
Glycogen storage disease in a young cat with heart failure.J Vet Intern Med. 2022 Jan;36(1):259-263. doi: 10.1111/jvim.16339. Epub 2021 Dec 23. J Vet Intern Med. 2022. PMID: 34939226 Free PMC article.
-
Clinical Insights Into Heritable Cardiomyopathies.Front Genet. 2021 Apr 28;12:663450. doi: 10.3389/fgene.2021.663450. eCollection 2021. Front Genet. 2021. PMID: 33995492 Free PMC article. Review.
-
Non-Progressive Hepatic Form of Andersen Disease as a Mimic of Hypertrophic Cardiomyopathy.Arq Bras Cardiol. 2020 Nov;115(5):964-966. doi: 10.36660/abc.20200218. Arq Bras Cardiol. 2020. PMID: 33295467 Free PMC article. English, Portuguese. No abstract available.
References
-
- Sipe JD, Benson MD, Buxbaum JN, Ikeda SI, Merlini G, Saraiva MJ, Westermark P. Amyloid fibril proteins and amyloidosis: chemical identification and clinical classification International Society of Amyloidosis 2016 Nomenclature Guidelines. Amyloid. 2016;23(4):209–213. - PubMed
-
- González-López E, Gagliardi C, Dominguez F, Quarta CC, de Haro-Del Moral FJ, Milandri A, Salas C, Cinelli M, Cobo-Marcos M, Lorenzini M, Lara-Pezzi E, Foffi S, Alonso-Pulpon L, Rapezzi C, Garcia-Pavia P. Clinical characteristics of wild-type transthyretin cardiac amyloidosis: disproving myths. Eur Heart J. 2017;38(24):1895–1904. - PubMed
-
- Castaño A, Narotsky DL, Hamid N, Khalique OK, Morgenstern R, DeLuca A, Rubin J, Chiuzan C, Nazif T, Vahl T, George I, Kodali S, Leon MB, Hahn R, Bokhari S, Maurer MS. Unveiling transthyretin cardiac amyloidosis and its predictors among elderly patients with severe aortic stenosis undergoing transcatheter aortic valve replacement. Eur Heart J. 2017;38(38):2879–2887. - PMC - PubMed
-
- Bennani Smires Y, Victor G, Ribes D, Berry M, Cognet T, Méjean S, et al. Pilot study for left ventricular imaging phenotype of patients over 65 years old with heart failure and preserved ejection fraction: the high prevalence of amyloid cardiomyopathy. Int J Card Imaging. 2016;32:1403–13. - PubMed
Publication types
LinkOut - more resources
Full Text Sources