

Outcome for pediatric acute promyelocytic leukemia patients at Children's Oncology Group sites on the Leukemia Intergroup Study CALGB 9710 (Alliance)
- PMID: 30393935
- PMCID: PMC6392047
- DOI: 10.1002/pbc.27542
Outcome for pediatric acute promyelocytic leukemia patients at Children's Oncology Group sites on the Leukemia Intergroup Study CALGB 9710 (Alliance)
Abstract
Background: Acute promyelocytic leukemia (APL) is a unique leukemia subtype requiring specialized treatment including all-trans retinoic acid (ATRA). A prior report demonstrated worse outcome among young children <5 years old compared with older children.
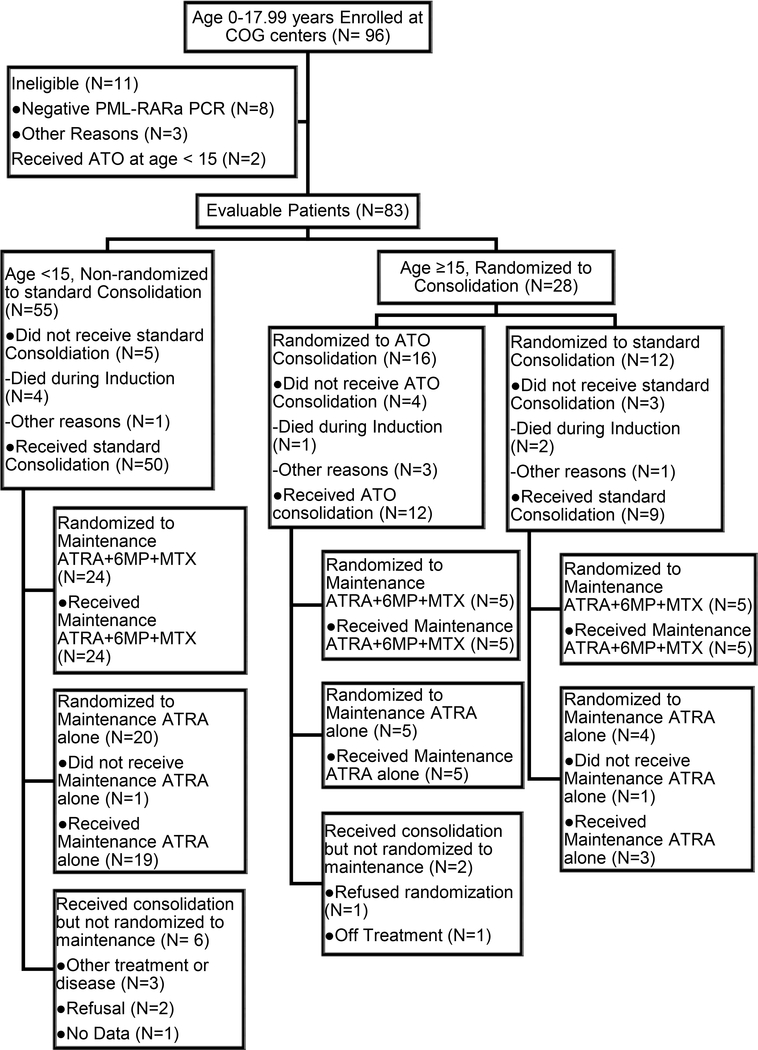
Methods: We evaluated outcomes for pediatric patients (<18 years old; N = 83) with APL treated on North American intergroup study CALGB 9710 at Children's Oncology Group sites. Induction and consolidation included ATRA, cytarabine, and anthracyclines. Patients ≥15 years old were randomized to addition of arsenic trioxide (ATO) consolidation. All patients were randomized to ATRA maintenance with versus without oral chemotherapy.
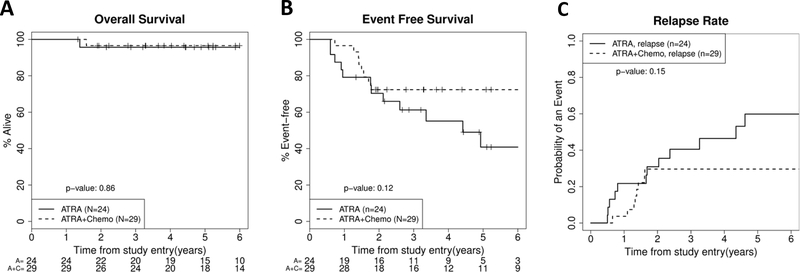
Results: The estimated 5-year overall survival (OS) rate was 82%, and the event-free survival (EFS) rate was 54%. Seven patients (8.4%) died during induction due to coagulopathy. Maintenance randomization demonstrated that addition of oral chemotherapy to ATRA significantly reduced relapse rate, but difference in EFS did not reach statistical significance (P = 0.12; 5-year rates [95% CI]: 41% [17%-64%] ATRA only vs 72% [56%-88%] ATRA plus chemotherapy). There was no difference (P = 0.93) in EFS for age <5 years versus 5-12.99 years versus 13-17.99 years (5-year rates: 56%, 47%, and 45%, respectively). Among adolescents 15-17.99 years old in the ATO randomization, there was a significantly lower relapse risk at 5 years for those receiving ATO (0% ATO vs 44% no ATO; P = 0.02).
Conclusion: Our data demonstrate that intensified ATRA, cytarabine, and anthracycline chemotherapy is effective for pediatric APL including very young patients, but early deaths and relapses remain barriers to cure. Further improvements are likely with incorporation of ATO into pediatric APL regimens.
Keywords: APL; ATRA; arsenic trioxide; pediatric.
© 2018 Wiley Periodicals, Inc.
Conflict of interest statement
Conflicts of Interest
The authors declare no competing financial interests.
Figures



References
-
- Gregory J, Kim H, Alonzo T, Gerbing R, Woods W, Weinstein H, Shepherd L, Schiffer C, Appelbaum F, Willman C, Wiernik P, Rowe J, Tallman M, Feusner J. Treatment of children with acute promyelocytic leukemia: results of the first North American Intergroup trial INT0129. Pediatr Blood Cancer 2009:53(6):1005–1010. - PMC - PubMed
-
- Lehmann S, Ravn A, Carlsson L, Antunovic P, Deneberg S, Mollgard L, Derolf AR, Stockelberg D, Tidefelt U, Wahlin A, Wennstrom L, Hoglund M, Juliusson G. Continuing high early death rate in acute promyelocytic leukemia: a population-based report from the Swedish Adult Acute Leukemia Registry. Leukemia 2011:25(7):1128–1134. - PubMed
-
- de la Serna J, Montesinos P, Vellenga E, Rayon C, Parody R, Leon A, Esteve J, Bergua JM, Milone G, Deben G, Rivas C, Gonzalez M, Tormo M, Diaz-Mediavilla J, Gonzalez JD, Negri S, Amutio E, Brunet S, Lowenberg B, Sanz MA. Causes and prognostic factors of remission induction failure in patients with acute promyelocytic leukemia treated with all-trans retinoic acid and idarubicin. Blood 2008:111(7):3395–3402. - PubMed
-
- Mandelli F, Diverio D, Avvisati G, Luciano A, Barbui T, Bernasconi C, Broccia G, Cerri R, Falda M, Fioritoni G, Leoni F, Liso V, Petti MC, Rodeghiero F, Saglio G, Vegna ML, Visani G, Jehn U, Willemze R, Muus P, et al. Molecular remission in PML/RAR alpha-positive acute promyelocytic leukemia by combined all-trans retinoic acid and idarubicin (AIDA) therapy. Gruppo Italiano-Malattie Ematologiche Maligne dell’Adulto and Associazione Italiana di Ematologia ed Oncologia Pediatrica Cooperative Groups. Blood 1997:90(3):1014–1021. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10CA031946/CA/NCI NIH HHS/United States
- U10CA180836/CA/NCI NIH HHS/United States
- U10 CA031946/CA/NCI NIH HHS/United States
- U10 CA033601/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- U10CA003927/CA/NCI NIH HHS/United States
- U10 CA180836/CA/NCI NIH HHS/United States
- U10CA180882/CA/NCI NIH HHS/United States
- U10CA041287/CA/NCI NIH HHS/United States
- U10CA033601/CA/NCI NIH HHS/United States
- U10 CA041287/CA/NCI NIH HHS/United States
- U10CA180886/CA/NCI NIH HHS/United States
- U10 CA180882/CA/NCI NIH HHS/United States
- U10 CA098543/CA/NCI NIH HHS/United States
- U10 CA180886/CA/NCI NIH HHS/United States
- U10CA180821/CA/NCI NIH HHS/United States
- U10 CA003927/CA/NCI NIH HHS/United States
- U10CA098543/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
