

Non-uraemic calciphylaxis successfully treated with pamidronate infusion
- PMID: 30393969
- PMCID: PMC7948727
- DOI: 10.1111/iwj.13019
Non-uraemic calciphylaxis successfully treated with pamidronate infusion
Abstract
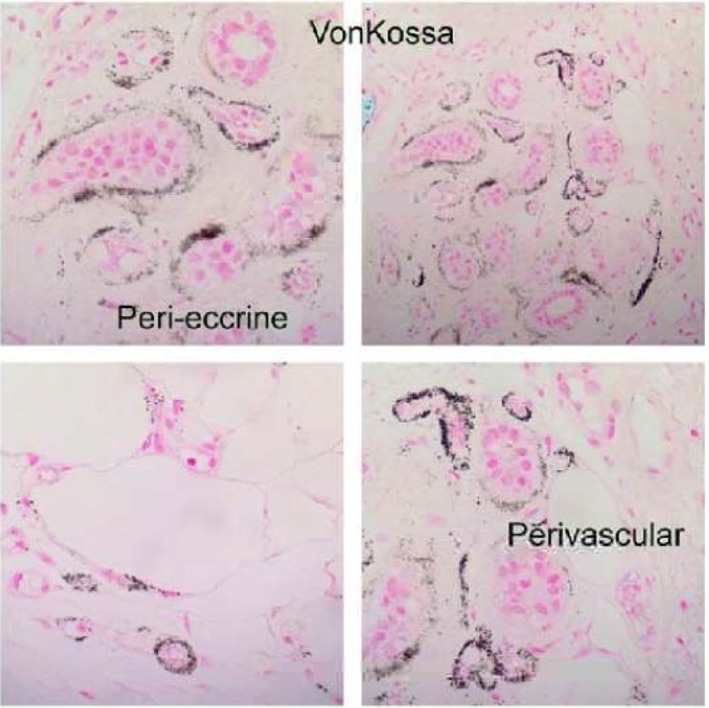
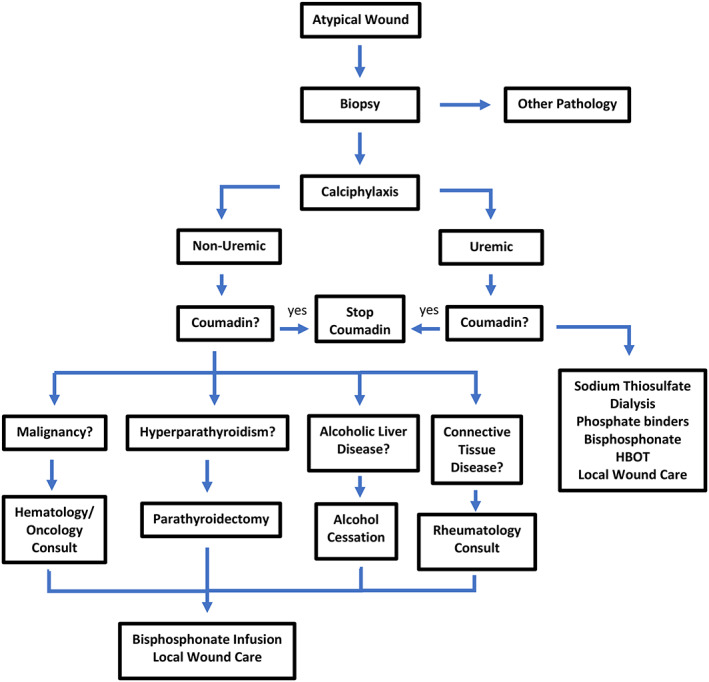
Calciphylaxis is a rare and potentially fatal disease that affects the subcutaneous layer of the skin. It is a calcific vasculopathy induced by a systemic process that causes occlusion of small blood vessels. The mortality rate for individuals diagnosed with calciphylaxis is estimated between 52% and 81% with sepsis being the leading cause of death. Uraemic calciphylaxis and its known effective treatments are well documented in the literature. Unfortunately, there is no known effective treatment for non-uraemic calciphylaxis. Most of the current treatments for non-uraemic calciphylaxis are derived from uraemic calciphylaxis treatment protocols. We report a case of a 75-year-old female with calciphylaxis on the right lower extremity who was successfully treated with four pamidronate infusions in addition to local wound care. This case represents a non-uraemic calciphylaxis wound successfully treated with pamidronate infusions and standard wound care, and suggests that IV pamidronate can be an effective treatment option.
Keywords: calcific arteriolopathy; leg ulcer; non-healing wound; sodium thiosulphate; vascular calcifications.
© 2018 Medicalhelplines.com Inc and John Wiley & Sons Ltd.
Conflict of interest statement
Disclosure
None reported.
Figures







Similar articles
-
Sodium thiosulfate and pamidronate for treatment of calciphylaxis: case report.Colomb Med (Cali). 2018 Dec 30;49(4):288-291. doi: 10.25100/cm.v49i3.4134. Colomb Med (Cali). 2018. PMID: 30700922 Free PMC article.
-
Multifaceted approach to a rare clinical case of calciphylaxis in a renal transplant recipient.G Ital Nefrol. 2019 Sep 24;36(5):2019-vol5. G Ital Nefrol. 2019. PMID: 31580546
-
Calcific uraemic arteriolopathy (calciphylaxis): data from a large nationwide registry.Nephrol Dial Transplant. 2017 Jan 1;32(1):126-132. doi: 10.1093/ndt/gfv438. Nephrol Dial Transplant. 2017. PMID: 26908770
-
Calciphylaxis in patients with chronic kidney disease: A disease which is still bewildering and potentially fatal.Nefrologia (Engl Ed). 2018 Nov-Dec;38(6):579-586. doi: 10.1016/j.nefro.2018.05.007. Epub 2018 Nov 8. Nefrologia (Engl Ed). 2018. PMID: 30415999 Review. English, Spanish.
-
Calciphylaxis: calcific uraemic arteriolopathy--a case study.J Ren Care. 2007 Apr-Jun;33(2):74-7. doi: 10.1111/j.1755-6686.2007.tb00044.x. J Ren Care. 2007. PMID: 17702510 Review.
Cited by
-
Cannabinoids in Integumentary Wound Care: A Systematic Review of Emerging Preclinical and Clinical Evidence.Pharmaceutics. 2024 Aug 17;16(8):1081. doi: 10.3390/pharmaceutics16081081. Pharmaceutics. 2024. PMID: 39204426 Free PMC article. Review.
-
Clinical characteristics and treatment modalities in uremic and non uremic calciphylaxis - a dermatological single-center experience.Ren Fail. 2024 Dec;46(1):2297566. doi: 10.1080/0886022X.2023.2297566. Epub 2024 Jan 4. Ren Fail. 2024. PMID: 38178572 Free PMC article.
-
Autologous platelet-rich plasma therapy for skin ulceration due to calcific uremic arteriopathy: a case report and review of the literature.Int Urol Nephrol. 2025 Apr 12. doi: 10.1007/s11255-025-04502-5. Online ahead of print. Int Urol Nephrol. 2025. PMID: 40220119
-
Calciphylaxis in end-stage kidney disease: outcome data from the United Kingdom Calciphylaxis Study.J Nephrol. 2021 Oct;34(5):1537-1545. doi: 10.1007/s40620-020-00908-9. Epub 2021 Feb 6. J Nephrol. 2021. PMID: 33548054 Free PMC article.
-
Topical cannabis-based medicines - A novel paradigm and treatment for non-uremic calciphylaxis leg ulcers: An open label trial.Int Wound J. 2020 Oct;17(5):1508-1516. doi: 10.1111/iwj.13484. Epub 2020 Sep 2. Int Wound J. 2020. PMID: 32875692 Free PMC article. Clinical Trial.
References
-
- Ning MS, Dahir KM, Castellanos EH, McGirt LY. Sodium thiosulfate in the treatment of non‐uremic calciphylaxis. J Dermatol. 2013;40(8):649‐652. - PubMed
-
- Vicco MH, Ferini F, Rodeles L, Baretta M, Marcipar I, Bottasso OA. Non‐uremic calciphylaxis and chagas disease. Rev Clin Esp (Barc). 2014;214(5):55. - PubMed
-
- Nigwekar SU. Multidisciplinary approach to calcific uremic arteriolopathy. Curr Opin Nephrol Hypertens. 2015;24(6):531‐537. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
