

Association of polymorphic variants in serotonin re-uptake transporter gene with Crohn's disease: a retrospective case-control study
- PMID: 30394015
- PMCID: PMC6240826
- DOI: 10.3325/cmj.2018.59.232
Association of polymorphic variants in serotonin re-uptake transporter gene with Crohn's disease: a retrospective case-control study
Abstract
Aim: To analyze the distribution of SLC6A4 gene polymorphisms in Crohn's disease (CD) patients and their association with the disease.
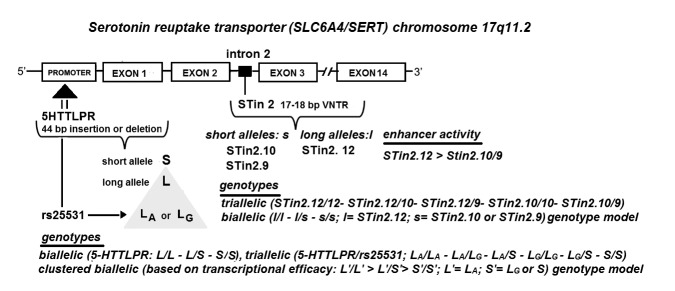
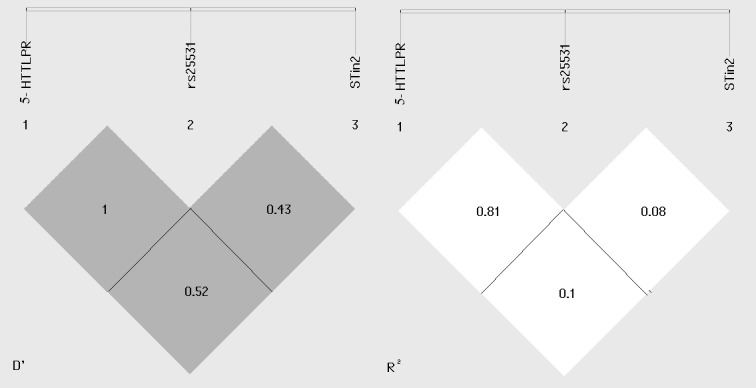
Methods: We evaluated the presence/absence of promoter (5-HTTLPR, rs25531) and intron 2 (STin2 VNTR) polymorphic variants of SLC6A4 gene in a retrospective case-control study including 192 CD patients and 157 healthy controls (HC). Genotyping was performed by polymerase chain reaction. The association of polymorphisms with CD and its clinical subtypes was analyzed using χ2 and Fisher exact test, binary logistic regression, and haplotype analysis.
Results: CD patients and healthy controls had similar sex (88 [45.8%] vs 84 [53.5%] women, respectively; P=0.154) and age (41.3±12.8 years vs 41.7±8.8 years, respectively, P=0.091) distribution. Significant differences were observed in the STin2 genotype and allele distribution between CD patients and healthy controls (P=0.003 and P=0.002, respectively) and between the corresponding female subgroups (P=0.004 and P=0.007, respectively), with a significant negative association of biallelic ss (STin2.9 and Stin2.10) STin2 genotype with CD (P=0.013, age- and sex-adjusted odds ratio [OR] 0.5, 95% confidence interval [CI] 0.29-0.86; women: P=0.006, age-adjusted OR 0.32, 95% CI 0.14-0.72) and a significantly higher S-STin2.12 (5-HTTLPR/rs25531: S-STin2: STin2.12) haplotype distribution in CD patients (P=0.004, OR 1.62, 95% CI 1.16-2.26). There was no significant association between 5-HTTLRP and rs25531 genotype or allele frequencies and CD and between any SLC6A4 polymorphic loci with clinical CD subtypes.
Conclusion: STin2 VNTR polymorphism of SLC6A4 gene may contribute to CD pathogenesis.
Figures
Similar articles
-
Genetic variants of SLC6A4 and risk of coronary artery disease: insights from North Indian population.Orphanet J Rare Dis. 2025 May 14;20(1):229. doi: 10.1186/s13023-025-03761-w. Orphanet J Rare Dis. 2025. PMID: 40369544 Free PMC article.
-
Association of serotonin transporter gene polymorphisms with poststroke depression.Arch Gen Psychiatry. 2008 Nov;65(11):1296-302. doi: 10.1001/archpsyc.65.11.1296. Arch Gen Psychiatry. 2008. PMID: 18981341 Free PMC article.
-
Study of the association of serotonin transporter triallelic 5-HTTLPR and STin2 VNTR polymorphisms with lithium prophylaxis response in bipolar disorder.Psychiatr Genet. 2013 Apr;23(2):77-81. doi: 10.1097/YPG.0b013e32835d6fad. Psychiatr Genet. 2013. PMID: 23277128
-
Role of the 5-HTTLPR and SNP Promoter Polymorphisms on Serotonin Transporter Gene Expression: a Closer Look at Genetic Architecture and In Vitro Functional Studies of Common and Uncommon Allelic Variants.Mol Neurobiol. 2016 Oct;53(8):5510-26. doi: 10.1007/s12035-015-9409-6. Epub 2015 Oct 13. Mol Neurobiol. 2016. PMID: 26464328 Review.
-
STin2 VNTR polymorphism in the serotonin transporter gene and migraine: pooled and meta-analyses.J Headache Pain. 2010 Aug;11(4):317-26. doi: 10.1007/s10194-010-0230-3. Epub 2010 Jun 29. J Headache Pain. 2010. PMID: 20585826 Free PMC article. Review.
Cited by
-
Interplay between Serotonin, Immune Response, and Intestinal Dysbiosis in Inflammatory Bowel Disease.Int J Mol Sci. 2022 Dec 9;23(24):15632. doi: 10.3390/ijms232415632. Int J Mol Sci. 2022. PMID: 36555276 Free PMC article. Review.
-
The Immune Landscape and Molecular Subtypes of Pediatric Crohn's Disease: Results from In Silico Analysis.J Pers Med. 2023 Mar 23;13(4):571. doi: 10.3390/jpm13040571. J Pers Med. 2023. PMID: 37108957 Free PMC article.
-
Predicting anxiety-related personality traits by means of serotonergic VNTR variants STin2 and 5-HTTLPR.J Mood Anxiety Disord. 2023 Oct 7;4:100031. doi: 10.1016/j.xjmad.2023.100031. eCollection 2023 Dec. J Mood Anxiety Disord. 2023. PMID: 40656971 Free PMC article.
References
-
- Burisch J. Crohn’s disease and ulcerative colitis. Occurrence, course and prognosis during the first year of disease in a European population-based inception cohort. Dan Med J. 2014;61:B4778. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical