

Tall Stature: A Challenge for Clinicians
- PMID: 30394212
- PMCID: PMC6696825
- DOI: 10.2174/1573396314666181105092917
Tall Stature: A Challenge for Clinicians
Abstract
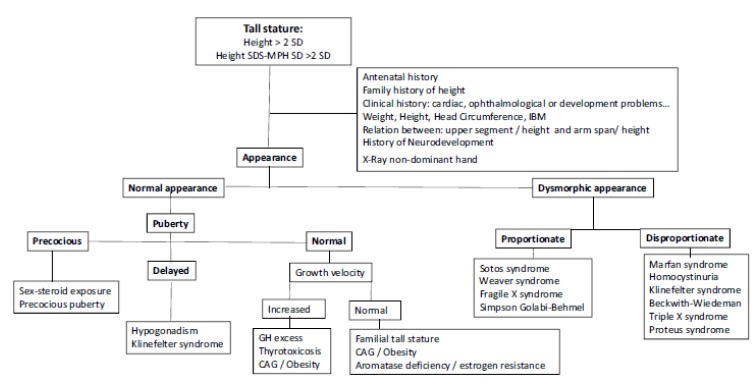
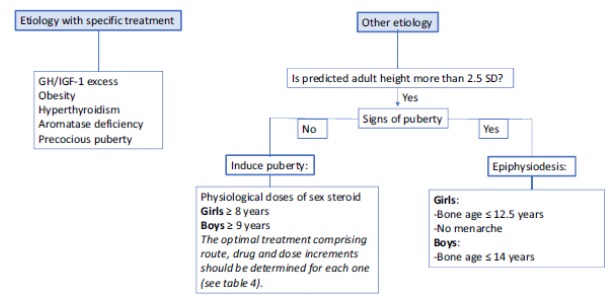
Clinicians generally use the term "tall stature" to define a height more than two standard deviations above the mean for age and sex. In most cases, these subjects present with familial tall stature or a constitutional advance of growth which is diagnosed by excluding the other conditions associated with overgrowth. Nevertheless, it is necessary to be able to identify situations in which tall stature or an accelerated growth rate indicate an underlying disorder. A careful physical evaluation allows the classification of tall patients into two groups: those with a normal appearance and those with an abnormal appearance including disproportion or dysmorphism. In the first case, the growth rate has to be evaluated and, if it is normal for age and sex, the subjects may be considered as having familial tall stature or constitutional advance of growth or they may be obese, while if the growth rate is increased, pubertal status and thyroid function should be evaluated. In turn, tall subjects having an abnormal appearance can be divided into proportionate and disproportionate syndromic patients. Before initiating further investigations, the clinician needs to perform both a careful physical examination and growth evaluation. To exclude pathological conditions, the cause of tall stature needs to be considered, although most children are healthy and generally do not require treatment to inhibit growth progression. In particular cases, familial tall stature subject can be treated by inducing puberty early and leading to a complete fusion of the epiphyses, so final height is reached. This review aims to provide proposals about the management of tall children.
Keywords: Tall stature; challenge; clinicians; disproportionate syndromes; proportionate syndromes; puberty..
Copyright© Bentham Science Publishers; For any queries, please email at epub@benthamscience.net.
Figures
Similar articles
-
Tall stature: a difficult diagnosis?Ital J Pediatr. 2017 Aug 3;43(1):66. doi: 10.1186/s13052-017-0385-5. Ital J Pediatr. 2017. PMID: 28774346 Free PMC article. Review.
-
How to investigate a child with excessive growth?Ann Endocrinol (Paris). 2017 Jun;78(2):98-103. doi: 10.1016/j.ando.2017.04.006. Epub 2017 May 5. Ann Endocrinol (Paris). 2017. PMID: 28483364 Review.
-
Tall stature in children and adolescents.Minerva Pediatr. 2020 Dec;72(6):472-483. doi: 10.23736/S0026-4946.20.05971-X. Epub 2020 Aug 4. Minerva Pediatr. 2020. PMID: 32748612 Review.
-
[Investigation of tall stature in children: Diagnostic work-up, review of the main causes].Arch Pediatr. 2018 Feb;25(2):163-169. doi: 10.1016/j.arcped.2017.12.010. Epub 2018 Feb 1. Arch Pediatr. 2018. PMID: 29395883 Review. French.
-
MANAGEMENT OF ENDOCRINE DISEASE: Diagnostic and therapeutic approach of tall stature.Eur J Endocrinol. 2017 Jun;176(6):R339-R353. doi: 10.1530/EJE-16-1054. Epub 2017 Mar 8. Eur J Endocrinol. 2017. PMID: 28274950 Review.
Cited by
-
Exome sequencing of patients with syndromic tall stature reveals four novel candidate genes.Endocr Connect. 2025 Jul 15;14(7):e250137. doi: 10.1530/EC-25-0137. Print 2025 Jul 1. Endocr Connect. 2025. PMID: 40577202 Free PMC article.
-
Dante Alighieri (1265-1321): an "infernal" endocrinological observation.Hormones (Athens). 2022 Mar;21(1):185-187. doi: 10.1007/s42000-021-00336-9. Epub 2021 Nov 9. Hormones (Athens). 2022. PMID: 34755282 Review.
-
Epidemiology of disorders associated with tall stature in childhood: A 20-year birth cohort study.PLoS One. 2025 Apr 15;20(4):e0321798. doi: 10.1371/journal.pone.0321798. eCollection 2025. PLoS One. 2025. PMID: 40233073 Free PMC article.
-
Novel Homozygous MTHFR Variant Causing Homocystinuria: Subtle Phenotypic Clues in Carriers.AACE Endocrinol Diabetes. 2025 Apr 25;12(2):128-131. doi: 10.1016/j.aed.2025.04.007. eCollection 2025 Jul-Aug. AACE Endocrinol Diabetes. 2025. PMID: 40786998 Free PMC article.
-
Etiology and Clinical Profile of Patients with Tall Stature: A Single-Center Experience.Indian J Endocrinol Metab. 2020 Sep-Oct;24(5):428-433. doi: 10.4103/ijem.IJEM_360_20. Epub 2020 Nov 9. Indian J Endocrinol Metab. 2020. PMID: 33489849 Free PMC article.
References
-
- Backeljauw P., Dattani M., Cohen P., Rosenfeld R. In: Disorders of Growth Hormone/Insulin-Like Growth Factor. 4th Ed. Sperling M., editor. Pediatric endocrinology; Eselvier Philadelphia: 2014. pp. 299–405.
-
- Wei C., Gregory J.W. Physiology of normal growth. Paediatr. Child Health. 2009;19:236–240.
-
- Davies J.H., Cheetham T. Investigation and management of tall stature. Arch. Dis. Child. 2014;99:772–777. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
