

A study of axitinib, a VEGF receptor tyrosine kinase inhibitor, in children and adolescents with recurrent or refractory solid tumors: A Children's Oncology Group phase 1 and pilot consortium trial (ADVL1315)
- PMID: 30394521
- PMCID: PMC6289772
- DOI: 10.1002/cncr.31725
A study of axitinib, a VEGF receptor tyrosine kinase inhibitor, in children and adolescents with recurrent or refractory solid tumors: A Children's Oncology Group phase 1 and pilot consortium trial (ADVL1315)
Erratum in
-
Erratum.Cancer. 2019 Aug 15;125(16):2896. doi: 10.1002/cncr.32331. Epub 2019 Jun 17. Cancer. 2019. PMID: 31355932 No abstract available.
Abstract
Background: Axitinib is an oral small molecule that inhibits receptor tyrosine kinases vascular endothelial growth factor receptors 1 to 3. A phase 1 and pharmacokinetic (PK) trial evaluating axitinib was conducted in children with refractory solid tumors.
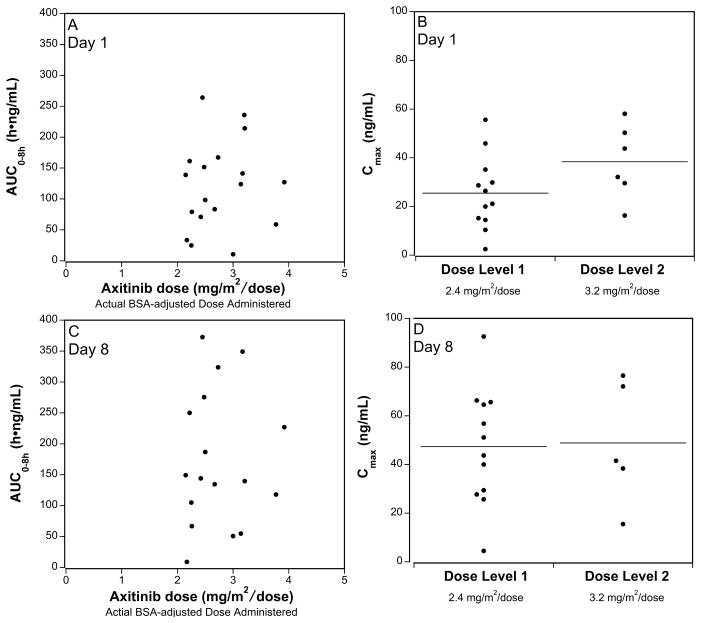
Methods: Axitinib was administered orally twice daily in continuous 28-day cycles. Dose levels (2.4 mg/m2 /dose and 3.2 mg/m2 /dose) were evaluated using a rolling 6 design. Serial PKs (cycle 1, days 1 and 8) and exploratory biomarkers were analyzed.
Results: A total of 19 patients were enrolled; 1 patient was ineligible due to inadequate time having elapsed from prior therapy. The median age of the patients was 13.5 years (range, 5-17 years). Two of 5 patients who were treated at dose level 2 experienced dose-limiting toxicities (palmar-plantar erythryodysesthesia syndrome in 1 patient and intratumoral hemorrhage in 1 patient). Frequent (>20%) grade 1 to 2 toxicities during cycle 1 included anemia, anorexia, fatigue, diarrhea, nausea, and hypertension. Nonhematological toxicities of grade ≥3 in subsequent cycles included hypertension and elevated serum lipase. PK analysis demonstrated variability in axitinib exposure, the median time to peak plasma concentration was 2 hours, and the half-life ranged from 0.7 to 5.2 hours. Exposure and dose were not found to be significantly associated with hypertension. Five patients achieved stable disease for ≤6 cycles as their best response, including patients with malignant peripheral nerve sheath tumor (1 patient), Ewing sarcoma (1 patient), hepatocellular carcinoma (1 patient), and osteosarcoma (2 patients). One patient with alveolar soft part sarcoma achieved a partial response. Kidney injury biomarkers were found to be elevated at baseline; no trends were identified.
Conclusions: In children with refractory solid tumors, the maximum tolerated and recommended dose of axitinib appears to be 2.4 mg/m2 /dose, which provides PK exposures similar to those of adults.
Keywords: Inlyta; axitinib; pediatric solid tumor; phase 1; vascular endothelial growth factor receptor (VEGFR).
© 2018 American Cancer Society.
Conflict of interest statement
Figures
References
-
- de Castro G, Junior, Puglisi F, de Azambuja E, et al. Angiogenesis and cancer: A cross-talk between basic science and clinical trials (the “do ut des” paradigm) Crit Rev Oncol Hematol. 2006;59:40–50. - PubMed
-
- Ferrara N. VEGF as a therapeutic target in cancer. Oncology. 2005;69(Suppl 3):11–6. - PubMed
-
- Hanahan D, Weinberg RA. The hallmarks of cancer. Cell. 2000;100:57–70. - PubMed
-
- Escudier B, Eisen T, Stadler WM, et al. Sorafenib in advanced clear-cell renal-cell carcinoma. Engl J Med. 2007;356:125–34. - PubMed
-
- Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359:378–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
