

Identifying high-cost episodes in lower extremity joint replacement
- PMID: 30394529
- PMCID: PMC6338304
- DOI: 10.1111/1475-6773.13078
Identifying high-cost episodes in lower extremity joint replacement
Abstract
Objectives: To evaluate the ability of claims-based risk adjustment and incremental components of clinical data to identify 90-day episode costs among lower extremity joint replacement (LEJR) patients according to the Centers for Medicare & Medicaid Services (CMS) Comprehensive Care for Joint Replacement (CJR) program provisions.
Data sources: Medicare fee-for-service (FFS) data for qualifying CJR episodes in the United States, and FFS data linked with clinical data from CJR-qualifying LEJR episodes performed at High Value Healthcare Collaborative (HVHC) and Mayo Clinic in 2013. HVHC and Mayo Clinic populations are subsets of the total FFS population to assess the additive value of additional pieces of clinical data in correctly assigning patients to cost groups.
Study design: Multivariable logistic models identified high-cost episodes.
Data collection/extraction methods: Clinical data from participating health care systems merged with Medicare FFS data.
Principal findings: Our three populations consisted of 363 621 patients in the CMS population, 4881 in the HVHC population, and 918 in the Mayo population. When modeling per CJR specifications, we observed low to moderate model performance (CMS C-Stat = 0.714; HVHC C-Stat = 0.628; Mayo C-Stat = 0.587). Adding CMS-HCC categories improved identification of patients in the top 20% of episode costs (CMS C-Stat = 0.758, HVHC C-Stat = 0.692, Mayo C-Stat = 0.677). Clinical variables, particularly functional status in the population for which this was available (Mayo C-Stat = 0.783), improved ability to identify patients within cost groups.
Conclusions: Policy makers could use these findings to improve payment adjustments for bundled LEJR procedures and in consideration of new data elements for reimbursement.
Keywords: health care expenditures; health care reform; medicare; reimbursement.
© Health Research and Educational Trust.
Figures
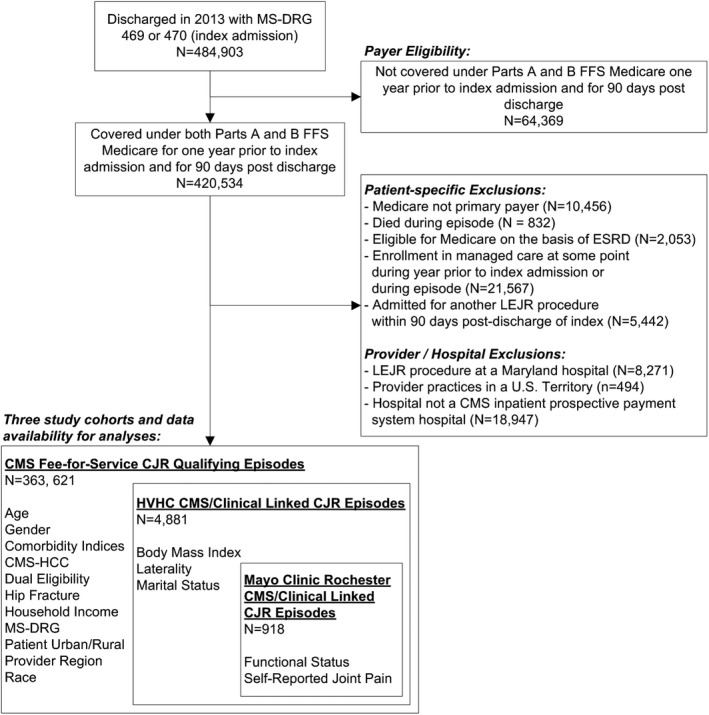
Note: Patient and Provider/Hospital Exclusions are not mutually exclusive; A single
LEJR episode may be excluded for more than one exclusion factor.
References
-
- Wolford ML, Palso K, Bercovitz A. Hospitalization for total hip replacement among inpatients aged 45 and over: United States, 2000‐2010. NCHS Data Brief. 2015;186:1‐8. - PubMed
-
- Williams SN, Wolford ML, Bercovitz A. Hospitalization for total knee replacement among inpatients aged 45 and over: United States, 2000‐2010. NCHS Data Brief. 2015;210:1‐8. - PubMed
-
- Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780‐785. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
