

Recommendations for the assessment and management of measurable residual disease in adults with acute lymphoblastic leukemia: A consensus of North American experts
- PMID: 30394566
- PMCID: PMC6572728
- DOI: 10.1002/ajh.25338
Recommendations for the assessment and management of measurable residual disease in adults with acute lymphoblastic leukemia: A consensus of North American experts
Abstract
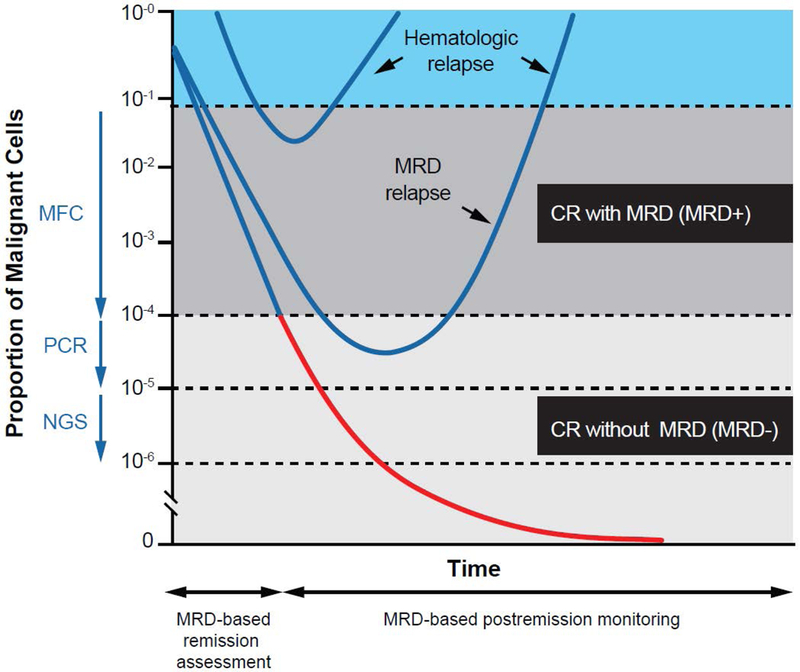
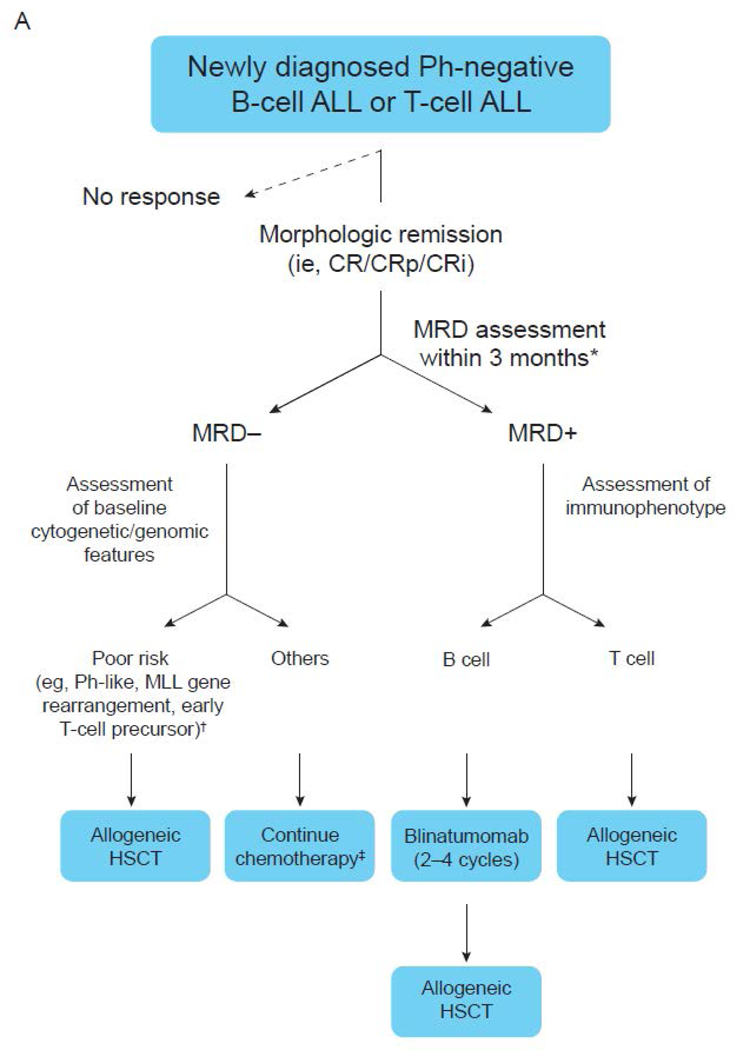
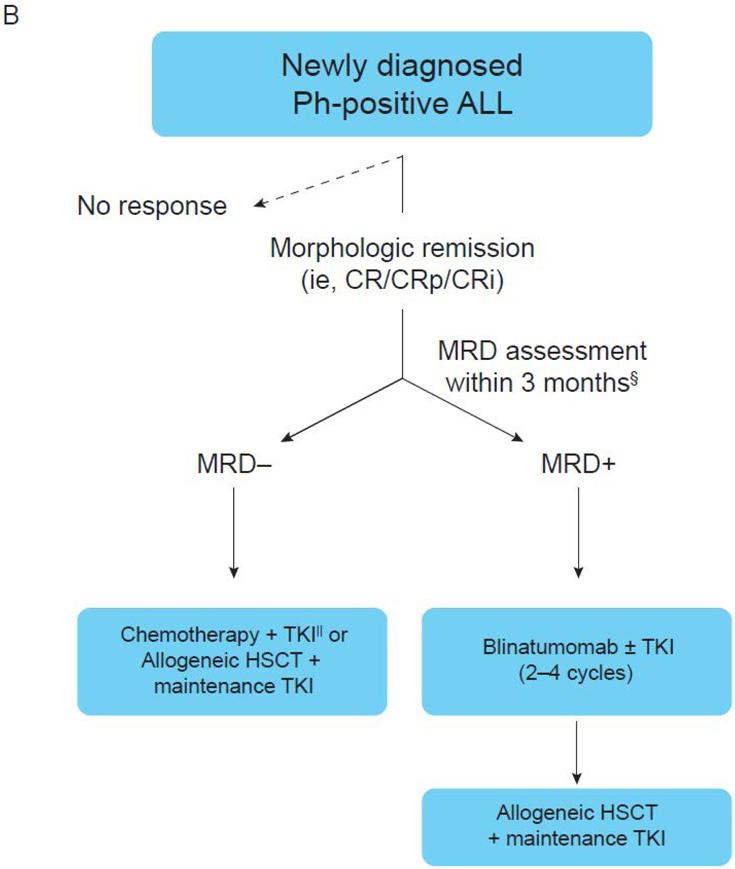
Measurable residual disease (MRD) that persists after initial therapy is a powerful predictor of relapse and survival in acute lymphoblastic leukemia (ALL). However, the optimal use of this information to influence therapeutic decisions is controversial. Herein, we comprehensively review the role of MRD assessment in adults with ALL, including methods to quantify residual leukemia cells during remission, prognostic impact of MRD across ALL subtypes, and available therapeutic approaches to eradicate MRD. This review presents consensus statements and provides an evidence-based framework for practicing hematologists and oncologists to use MRD information to make rational treatment decisions in adult patients with ALL.
© 2018 Wiley Periodicals, Inc.
Figures
Similar articles
-
How I Diagnose Minimal/Measurable Residual Disease in B Lymphoblastic Leukemia/Lymphoma by Flow Cytometry.Am J Clin Pathol. 2021 Jan 4;155(1):38-54. doi: 10.1093/ajcp/aqaa242. Am J Clin Pathol. 2021. PMID: 33236071 Review.
-
Measurable residual disease at myeloablative allogeneic transplantation in adults with acute lymphoblastic leukemia: a retrospective registry study on 2780 patients from the acute leukemia working party of the EBMT.J Hematol Oncol. 2019 Oct 23;12(1):108. doi: 10.1186/s13045-019-0790-x. J Hematol Oncol. 2019. PMID: 31647022 Free PMC article.
-
Characteristics and Therapeutic Targeting of Minimal Residual Disease in Childhood Acute Lymphoblastic Leukemia.Adv Exp Med Biol. 2018;1100:127-139. doi: 10.1007/978-3-319-97746-1_8. Adv Exp Med Biol. 2018. PMID: 30411264 Review.
-
Optimal Measurable Residual Disease Testing for Acute Myeloid Leukemia.Surg Pathol Clin. 2019 Sep;12(3):671-686. doi: 10.1016/j.path.2019.03.009. Epub 2019 May 18. Surg Pathol Clin. 2019. PMID: 31352980 Review.
-
Detection of minimal residual disease in pediatric acute lymphoblastic leukemia.Cytometry B Clin Cytom. 2013 Nov-Dec;84(6):359-69. doi: 10.1002/cyto.b.21101. Epub 2013 Jun 26. Cytometry B Clin Cytom. 2013. PMID: 23757107 Review.
Cited by
-
MRD-Based Therapeutic Decisions in Genetically Defined Subsets of Adolescents and Young Adult Philadelphia-Negative ALL.Cancers (Basel). 2021 Apr 27;13(9):2108. doi: 10.3390/cancers13092108. Cancers (Basel). 2021. PMID: 33925541 Free PMC article. Review.
-
Clinical trial update on bispecific antibodies, antibody-drug conjugates, and antibody-containing regimens for acute lymphoblastic leukemia.J Hematol Oncol. 2019 Feb 8;12(1):15. doi: 10.1186/s13045-019-0703-z. J Hematol Oncol. 2019. PMID: 30736842 Free PMC article. Review.
-
Evolving therapy of adult acute lymphoblastic leukemia: state-of-the-art treatment and future directions.J Hematol Oncol. 2020 Jun 5;13(1):70. doi: 10.1186/s13045-020-00905-2. J Hematol Oncol. 2020. PMID: 32503572 Free PMC article. Review.
-
Liquid biopsies and minimal residual disease in lymphoid malignancies.Front Oncol. 2023 May 9;13:1173701. doi: 10.3389/fonc.2023.1173701. eCollection 2023. Front Oncol. 2023. PMID: 37228488 Free PMC article. Review.
-
Immunophenotypic measurable residual disease monitoring in adult acute lymphoblastic leukemia patients undergoing allogeneic hematopoietic stem cell transplantation.Front Oncol. 2023 Feb 22;13:1047554. doi: 10.3389/fonc.2023.1047554. eCollection 2023. Front Oncol. 2023. PMID: 36910638 Free PMC article. Review.
References
-
- Bruggemann M, Raff T, Kneba M. Has MRD monitoring superseded other prognostic factors in adult ALL? Blood 2012; 120(23): 4470–81. - PubMed
-
- Bruggemann M, Raff T, Flohr T, et al. Clinical significance of minimal residual disease quantification in adult patients with standard-risk acute lymphoblastic leukemia. Blood 2006; 107(3): 1116–23. - PubMed
-
- Gokbuget N, Kneba M, Raff T, et al. Adult patients with acute lymphoblastic leukemia and molecular failure display a poor prognosis and are candidates for stem cell transplantation and targeted therapies. Blood 2012; 120(9): 1868–76. - PubMed