

Realistic 4D MRI abdominal phantom for the evaluation and comparison of acquisition and reconstruction techniques
- PMID: 30394573
- PMCID: PMC7728431
- DOI: 10.1002/mrm.27545
Realistic 4D MRI abdominal phantom for the evaluation and comparison of acquisition and reconstruction techniques
Abstract
Purpose: This work presents a 4D numerical abdominal phantom, which includes T1 and T2 relaxation times, proton density fat fraction, perfusion, and diffusion, as well as respiratory motion for the evaluation and comparison of acquisition and reconstruction techniques.
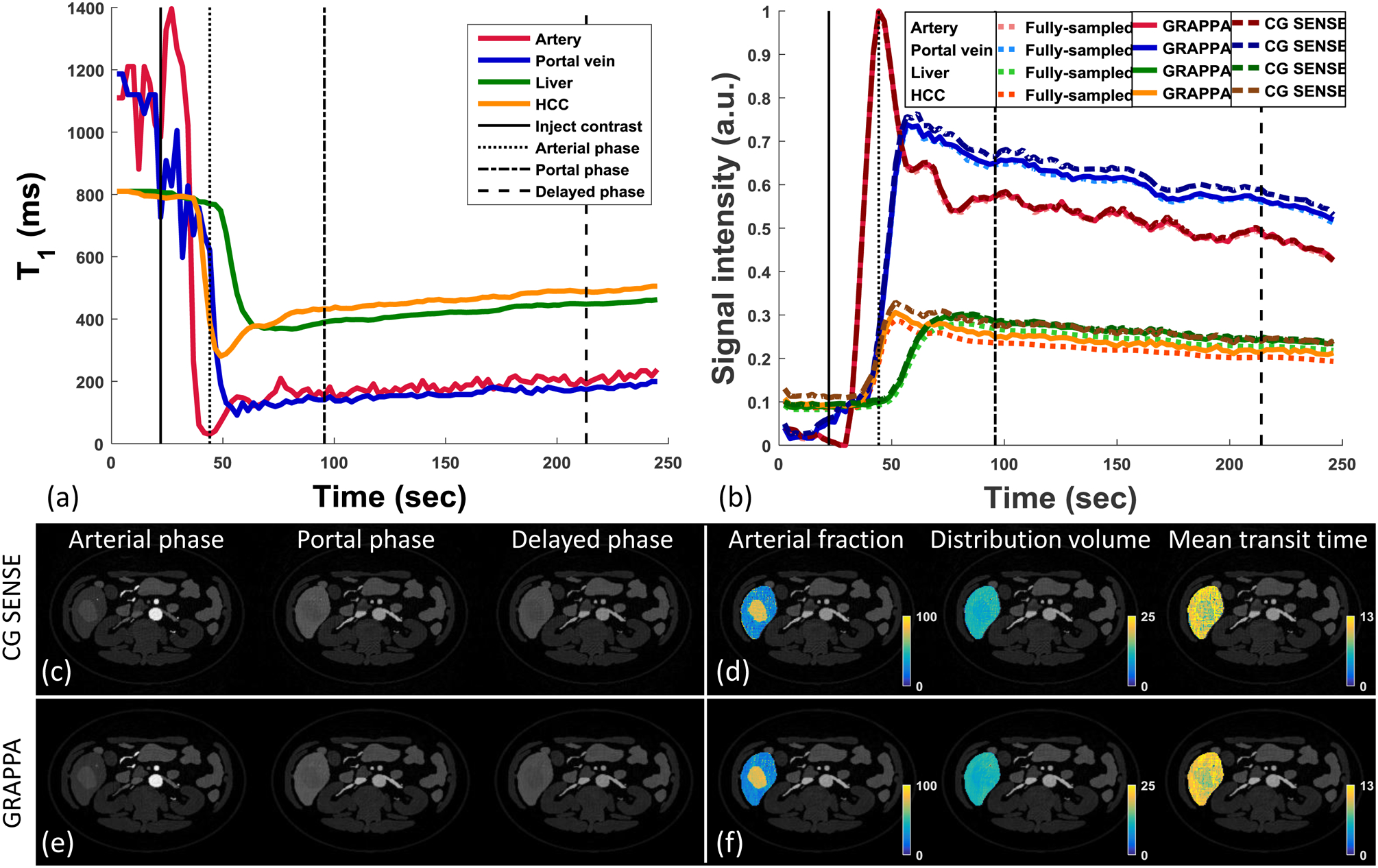
Methods: The 3D anatomical mesh models were non-rigidly scaled and shifted by respiratory motion derived from an in vivo scan. A time series of voxelized 3D abdominal phantom images were obtained with contrast determined by the tissue properties and pulse sequence parameters. Two example simulations: (1) 3D T1 mapping under breath-hold and free-breathing acquisition conditions and (2) two different reconstruction techniques for accelerated 3D dynamic contrast-enhanced MRI, are presented. The source codes can be found at https://github.com/SeiberlichLab/Abdominal_MR_Phantom.
Results: The proposed 4D abdominal phantom can successfully simulate images and MRI data with nonrigid respiratory motion and specific contrast settings and data sampling schemes. In example 1, the use of a numerical 4D abdominal phantom was demonstrated to aid in the comparison between different approaches for volumetric T1 mapping. In example 2, the average arterial fraction over the healthy hepatic parenchyma as calculated with spiral generalized autocalibrating partial parallel acquisition was closer to that from the fully sampled data than the arterial fraction from conjugate gradient sensitivity encoding, although both are elevated compared to the gold-standard reference.
Conclusion: This realistic abdominal MR phantom can be used to simulate different pulse sequences and data sampling schemes for the comparison of acquisition and reconstruction methods under controlled conditions that are impossible or prohibitively difficult to perform in vivo.
Keywords: MRI; abdomen; digital phantom; free breathing.
© 2018 International Society for Magnetic Resonance in Medicine.
Figures






References
-
- Chen Y, Lee GR, Wright KL, Badve C, Nakamoto D, Yu A, Schluchter MD, Griswold MA, Seiberlich N, Gulani V. Free-breathing liver perfusion imaging using 3-dimensional through-time spiral generalized autocalibrating partially parallel acquisition acceleration. Invest. Radiol 2015;50:367–375. doi: 10.1097/RLI.0000000000000135. - DOI - PMC - PubMed
-
- Cocosco C a, Kollokian V, Kwan RK, Pike GB, Evans AC. BrainWeb : Online Interface to a 3D MRI Simulated Brain Database. 3-rd Int. Conf. Funct. Mapp. Hum. Brain 1997;5:S425. doi: 10.1.1.51.3917.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
