

Thrombotic microangiopathy associated with gemcitabine use: Presentation and outcome in a national French retrospective cohort
- PMID: 30394581
- PMCID: PMC6339967
- DOI: 10.1111/bcp.13808
Thrombotic microangiopathy associated with gemcitabine use: Presentation and outcome in a national French retrospective cohort
Abstract
Aims: Gemcitabine has been associated with thrombotic microangiopathy (TMA). We conducted a national retrospective study of gemcitabine-associated TMA (G-TMA).
Methods: From 1998 to 2015, all cases of G-TMA reported to the French Pharmacovigilance Network and the French TMA Reference Center, and cases explored for complement alternative pathway abnormalities, were analysed.
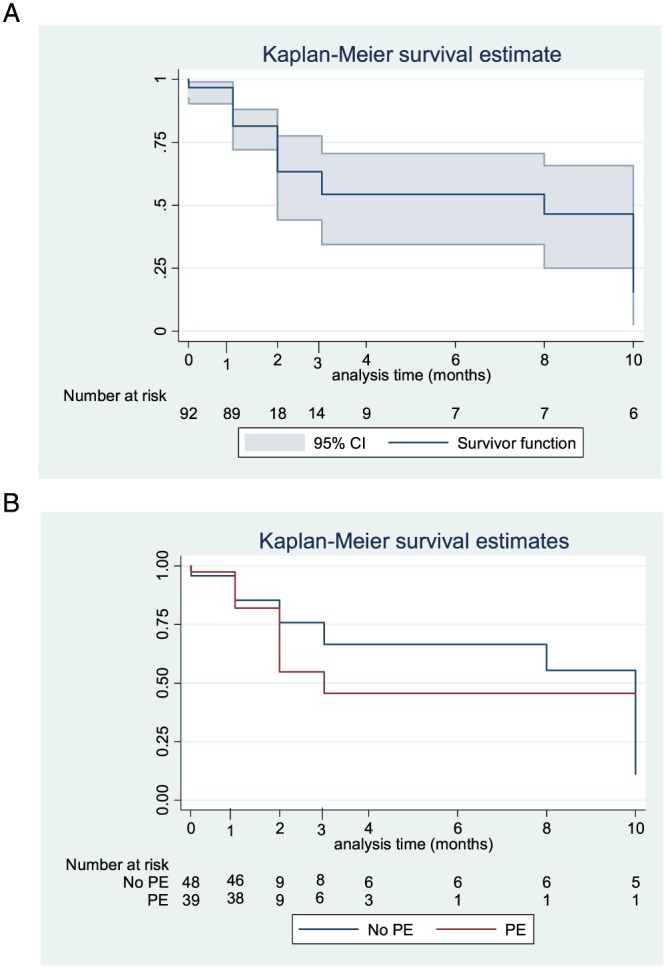
Results: G-TMA was diagnosed in 120 patients (median age 61.5 years), after a median of 210 days of treatment, and a cumulative dose of 12 941 mg m-2 . Gemcitabine indications were: pancreatic (52.9%), pulmonary (12.6%) and breast (7.6%) cancers, metastatic in 34.2% of cases. Main symptoms were oedema (56.7%) and new-onset or exacerbated hypertension (62.2%). Most patients presented with haemolytic anaemia (95.6%) and thrombocytopenia (74.6%). Acute kidney injury was reported in 97.4% and dialysis was required in 27.8% of patients. Treatment consisted of: plasma exchange (PE; 39.8%), fresh frozen plasma (21.4%), corticosteroids (15.3%) and eculizumab (5.1%). A complete remission of TMA was obtained in 42.1% of patients and haematological remission in 23.1%, while 34.7% did not improve. The survival status was known for 52 patients, with 29 deaths (54.7%). Patients treated with PE, despite a more severe acute kidney injury, requiring dialysis more frequently, displayed comparable rates of remission, but with more adverse events. No abnormality in complement alternative pathway was documented in patients explored.
Conclusion: This large cohort confirms the severity of G-TMA, associated with severe renal failure and death. Oedema and hypertension could be monitored in patients treated with gemcitabine to detect early TMA. The benefit of PE or eculizumab deserves further investigation.
Keywords: acute kidney injury; adverse drug reactions; chemotherapy; medication safety; pharmacovigilance.
© 2018 The British Pharmacological Society.
Figures
References
-
- Green MR. Gemcitabine safety overview. Semin Oncol 1996; 23 (5 Suppl. 10): 32–35. - PubMed
-
- Humphreys BD, Sharman JP, Henderson JM, Clark JW, Marks PW, Rennke HG, et al Gemcitabine‐associated thrombotic microangiopathy. Cancer 2004; 100: 2664–2670. - PubMed
-
- Izzedine H, Perazella MA. Thrombotic microangiopathy, cancer, and cancer drugs. Am J Kidney Dis 2015; 66: 857–868. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
