

doi: 10.1177/1591019918810850.
Epub 2018 Nov 4.
Surgical options in experimental porcine model for endovascular training in complex vascular lesions
Affiliations
- PMID: 30394842
- PMCID: PMC6547208
- DOI: 10.1177/1591019918810850
Item in Clipboard
Surgical options in experimental porcine model for endovascular training in complex vascular lesions
Interv Neuroradiol.
2019 Jun.
Abstract
We describe a new, elegant, two-phase, microsurgical method that minimizes the surgical preparation time for different complex vascular lesions in a swine model. In the first phase, the model is prepared microsurgically in the experimental laboratory using arterial or/and venous grafts. In the second phase, the model is implanted in the experimental animal. This two-fold method allows for increasing the complexity and accuracy of the model while reducing preparation time on the day of the training session.
Keywords: Endovascular training; aneurysm model; animal experimentation; arteriovenous fistula model; experimental surgery.
Figures
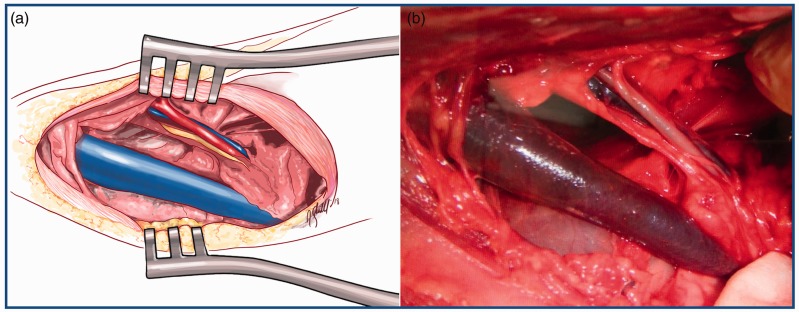
displays a schematic drawing (image a) and a surgical picture
(image b) of a cervical dissection and exposure of the
neurovascular bundle of the neck. This is the site of
implantation of the models. It includes the common carotid
artery, the vagosympathetic trunk and the internal jugular vein.
Of greater thickness, the external jugular vein is also exposed
in the dissection.
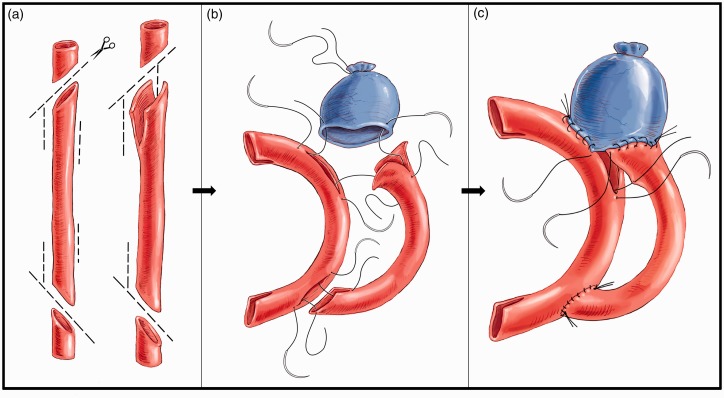
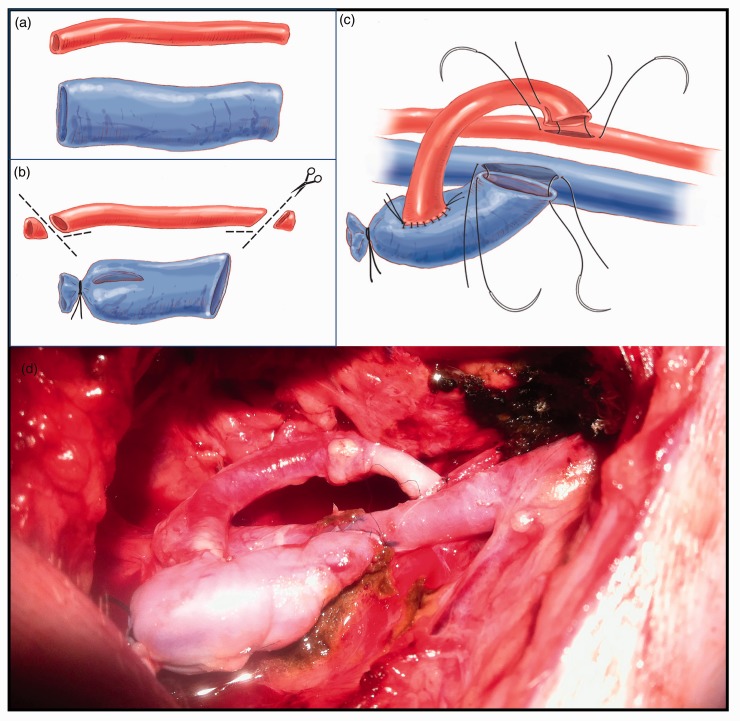
illustrates the construction of a complex wide-neck bifurcation
aneurysm. The purpose of this figure is to display schematically
how we perform the aneurysm reconstruction represented in Figure 3.
For the preparation of this complex model, we require the use of
two arterial grafts and one venous graft (image 2a). The first
arterial graft is used as a recipient of the second arterial
graft and part of the venous graft. For its subsequent
implementation, two oblique cuts are made at each end, as well
as two lateral slits (fish mouth). In this same artery two
lateral slits are made for the suturing of the second arterial
graft. In the second arterial graft, two oblique cuts and two
lateral slits are made to facilitate anastomosis to the first
graft. However, at the proximal end of this second graft
additional slits are made, the length of which determines the
neck of the aneurysm and the location of the base on one or both
branches. In other words, the shorter the upper groove in
relation to the lower one, the lower the aneurysm will be in
relation to this vessel. To carry out the anastomosis, the usual
technique is followed, in which anchorage is made at the margins
and a continuous suture is put under tension once all points
have been correctly passed (images 2b and 2c).
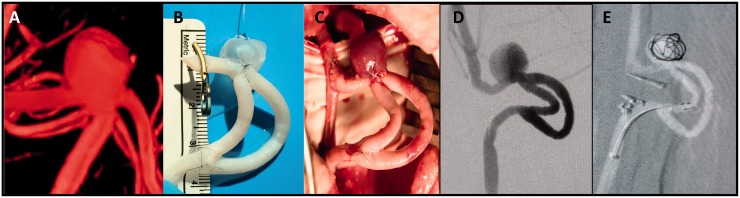
Image 3a corresponds to three-dimensional reconstruction of a
typical aneurysm at the bifurcation of the middle cerebral
artery. Note the amplitude of the neck of the aneurysm and its
preferential relationship with one of the two branches. In image
3b the created model is shown, ready for later implantation in
the experimental animal. Image 3c shows a surgical view of the
model just after implantation and image 3d corresponds to an
angiographic image of the final implanted model. Note the model
has all the angiographic characteristics of the desired
aneurysm. The created aneurysm has a wide base of implantation
with a preferential relationship to one of the branches. Image
3e shows an image of the practice in which partial embolization
of the aneurysm is observed. Note the two clips placed distally
to the first end-to-side anastomosis and proximally to the
second end-to-side anastomosis to occlude the carotid
artery.
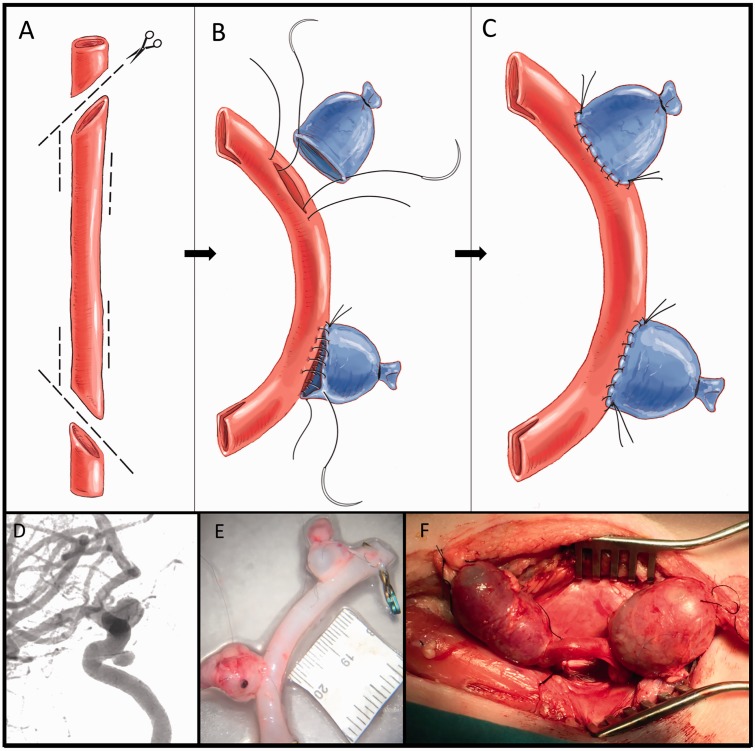
The figure shows the construction of two wide-neck aneurysms in a
cavernous carotid artery model. The object of the model is to
represent two aneurysms in an artery with the precise curvature
typical of the cavernous artery. This requires the use of one
arterial graft and one venous graft (image 4a). The arterial
graft is used as a recipient of the venous graft. For its
subsequent implementation in the carotid artery, two oblique
cuts with lateral slits (fish mouth) are made at each end. In
this same artery, two lateral slits are made for the
implantation of the venous grafts. The size of these lateral
slits determines the neck of the aneurysm and the size of the
selected vein dictates the size of the aneurismal dome. To carry
out the anastomosis, the usual technique is followed, anchoring
first at the margins and tensing a continuous suture once all
points have been correctly passed (images 4b and c). Image 4d
corresponds to a typical angiography of a wide-neck aneurysm of
the intracavernosal carotid artery. In image 4e the created
model is shown, ready for later implantation in the experimental
animal. Image 4f shows a surgical image of the model after
implantation.
The figure shows the construction of an arteriovenous fistula.
This requires the use of one arterial graft and one venous graft
(image 5a). As per protocol, two oblique cuts with lateral slits
(fish mouth) are made at each end. For the preparation of the
model, one end of the vein is occluded. A slit that matches the
diameter of the artery to be anastomosed is made (image 5b). The
arterial graft is connected laterally to the venous graft for
subsequent implementation on the carotid artery and internal
jugular vein (image 5c). To carry out the anastomosis, the usual
technique is followed: anchorage at the margins and tension of a
continuous suture once all tissue has been correctly passed.
Image 5d shows a surgical view of the arteriovenous model after
implementation.
References
-
- Arthur A, Hoit D, Coon A, et al. Physician training protocol within the WEB Intrasaccular Therapy (WEB-IT) study. J Neurointerventional Surg 2018; 10: 500–504. - PubMed
-
- Bavinzski G, al-Schameri A, Killer M, et al. Experimental bifurcation aneurysm: A model for in vivo evaluation of endovascular techniques. Minimally Invasive Neurosurg 1998; 41: 129–132. - PubMed
-
- Boulos AS, Deshaies EM, Fessler RD, et al. A triple bifurcation aneurysm model for evaluating complex endovascular therapies in dogs. J Neurosurg 2005; 103: 739–744. - PubMed
-
- da Silva SL, Jr, Pitta GB, Pereira AH, et al. Stable experimental model of carotid artery saccular aneurysm in swine using the internal jugular vein. Rev Col Bras Cir 2013; 40: 130–136. - PubMed
-
- Olabe J, Olabe J, Roda J. Microsurgical cerebral aneurysm training porcine model. Neurol India 2011; 59: 78–81. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
