

Comparison of Methods for Identification of Pediatric Severe Sepsis and Septic Shock in the Virtual Pediatric Systems Database
- PMID: 30394917
- PMCID: PMC6336511
- DOI: 10.1097/CCM.0000000000003541
Comparison of Methods for Identification of Pediatric Severe Sepsis and Septic Shock in the Virtual Pediatric Systems Database
Abstract
Objectives: To compare the performance of three methods of identifying children with severe sepsis and septic shock from the Virtual Pediatric Systems database to prospective screening using consensus criteria.
Design: Observational cohort study.
Setting: Single-center PICU.
Patients: Children admitted to the PICU in the period between March 1, 2012, and March 31, 2014.
Interventions: None.
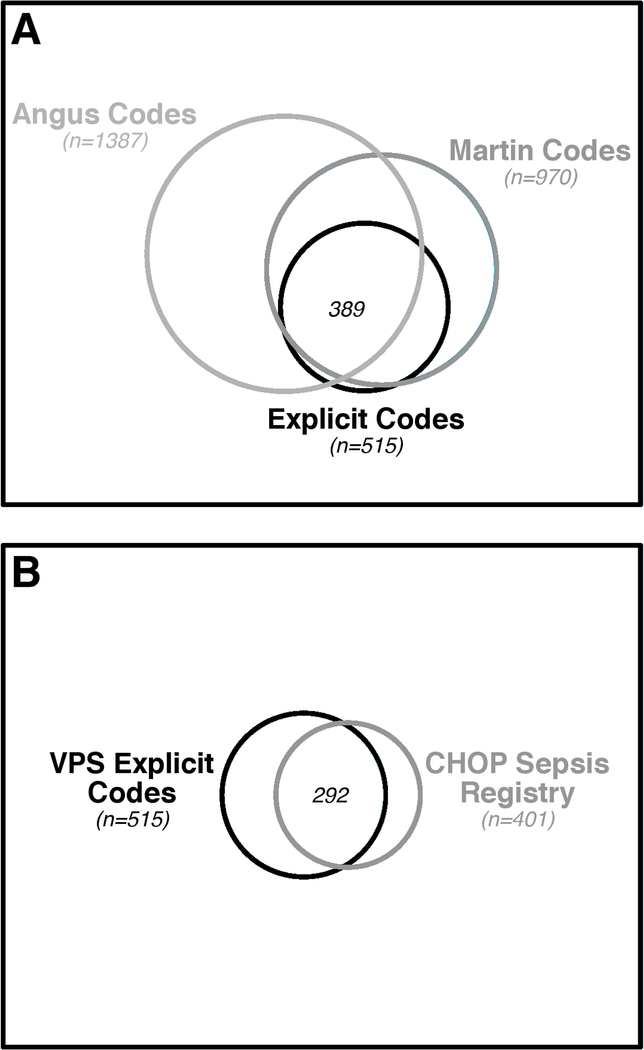
Measurements and main results: During the study period, all PICU patients were prospectively screened daily for sepsis, and those meeting consensus criteria for severe sepsis or septic shock on manual chart review were entered into the sepsis registry. Of 7,459 patients admitted to the PICU during the study period, 401 met consensus criteria for severe sepsis or septic shock (reference standard cohort). Within Virtual Pediatric Systems, patients identified using "Martin" (n = 970; κ = 0.43; positive predictive value = 34%; F1 = 0.48) and "Angus" International Classification of Diseases, 9th Edition, Clinical Modification codes (n = 1387; κ = 0.28; positive predictive value = 22%; F1 = 0.34) showed limited agreement with the reference standard cohort. By comparison, explicit International Classification of Diseases, 9th Edition, Clinical Modification codes for severe sepsis (995.92) and septic shock (785.52) identified a smaller, more accurate cohort of children (n = 515; κ = 0.61; positive predictive value = 57%; F1 = 0.64). PICU mortality was 8% in the reference standard cohort and the cohort identified by explicit codes; age, illness severity scores, and resource utilization did not differ between groups. Analysis of discrepancies between the reference standard and Virtual Pediatric Systems explicit codes revealed that prospective screening missed 66 patients with severe sepsis or septic shock. After including these patients in the reference standard cohort as an exploratory analysis, agreement between the cohort of patients identified by Virtual Pediatric Systems explicit codes and the reference standard cohort improved (κ = 0.73; positive predictive value = 70%; F1 = 0.75).
Conclusions: Children with severe sepsis and septic shock are best identified in the Virtual Pediatric Systems database using explicit diagnosis codes for severe sepsis and septic shock. The accuracy of these codes and level of clinical detail available in the Virtual Pediatric Systems database allow for sophisticated epidemiologic studies of pediatric severe sepsis and septic shock in this large, multicenter database.
Conflict of interest statement
Figures
Comment in
-
Sepsis Computable Phenotypes in the Service of Observational Research.Crit Care Med. 2019 Feb;47(2):303-305. doi: 10.1097/CCM.0000000000003564. Crit Care Med. 2019. PMID: 30653066 Free PMC article. No abstract available.
References
-
- Dellinger RP, Levy MM, Rhodes A, et al.: Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. 2013. p. 580–637. - PubMed
-
- Watson RS, Carcillo JA: Scope and epidemiology of pediatric sepsis. Pediatric Critical Care Medicine 2005; 6:S3–5 - PubMed
-
- Hartman ME, Linde-Zwirble WT, Angus DC, et al.: Trends in the epidemiology of pediatric severe sepsis*. Pediatric Critical Care Medicine 2013; 14:686–693 - PubMed
-
- Goldstein B, Giroir B, Randolph A, et al.: International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. 2005. p. 2–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
