

Biliary Bicarbonate, pH, and Glucose Are Suitable Biomarkers of Biliary Viability During Ex Situ Normothermic Machine Perfusion of Human Donor Livers
- PMID: 30395120
- PMCID: PMC6613725
- DOI: 10.1097/TP.0000000000002500
Biliary Bicarbonate, pH, and Glucose Are Suitable Biomarkers of Biliary Viability During Ex Situ Normothermic Machine Perfusion of Human Donor Livers
Abstract
Background: Ex situ normothermic machine perfusion (NMP) can be used to assess viability of suboptimal donor livers before implantation. Our aim was to assess the diagnostic accuracy of bile biochemistry for the assessment of bile duct injury (BDI).
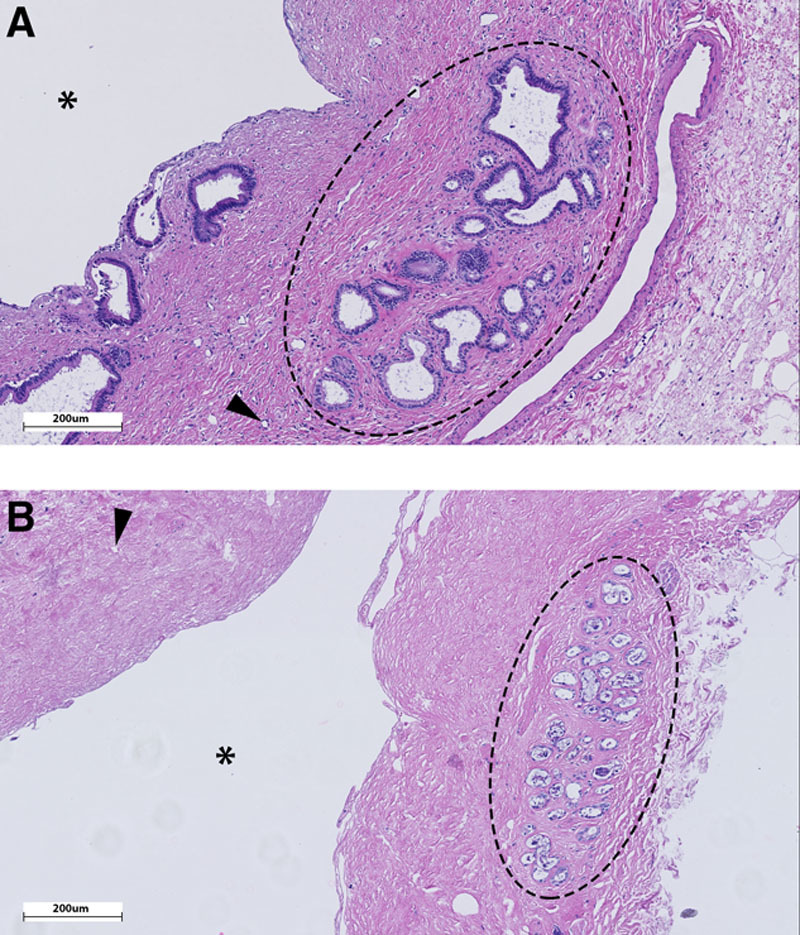
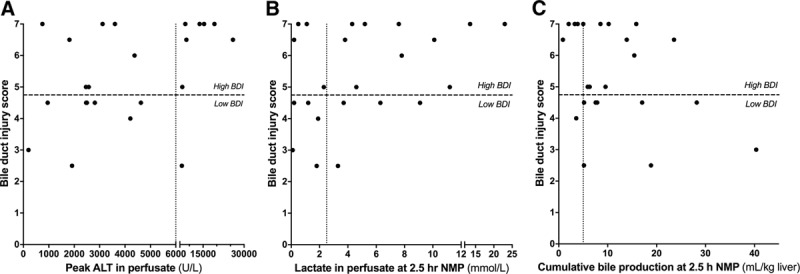
Methods: In a preclinical study, 23 human donor livers underwent 6 hours of end-ischemic NMP to determine biomarkers of BDI. Livers were divided into groups with low or high BDI, based on a clinically relevant histological grading system. During NMP, bile was analyzed biochemically and potential biomarkers were correlated with the degree of BDI. Receiver operating characteristics curves were generated to determine optimal cutoff values. For clinical validation, identified biomarkers were subsequently included as viability criteria in a clinical trial (n = 6) to identify transplantable liver grafts with low BDI.
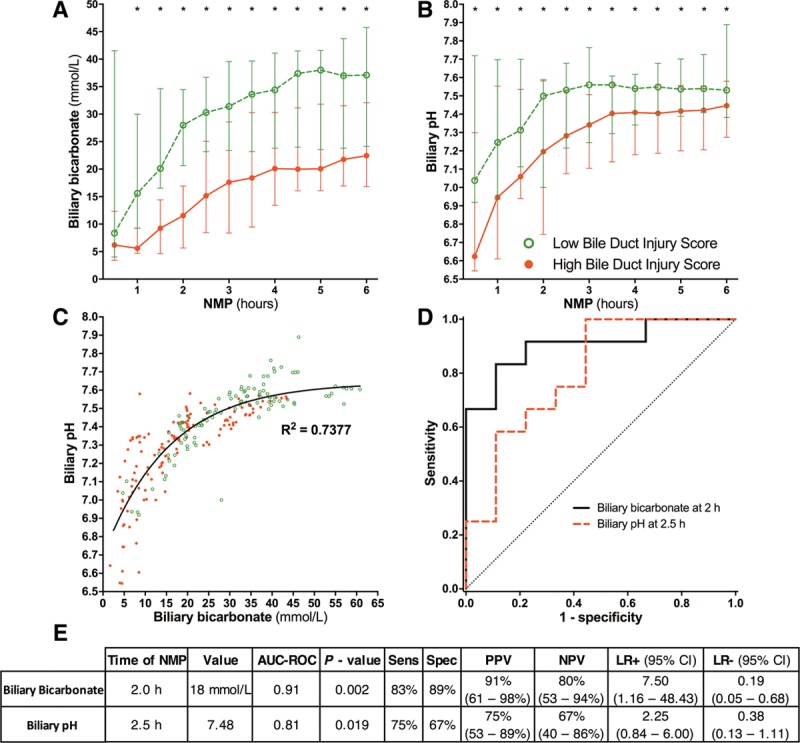
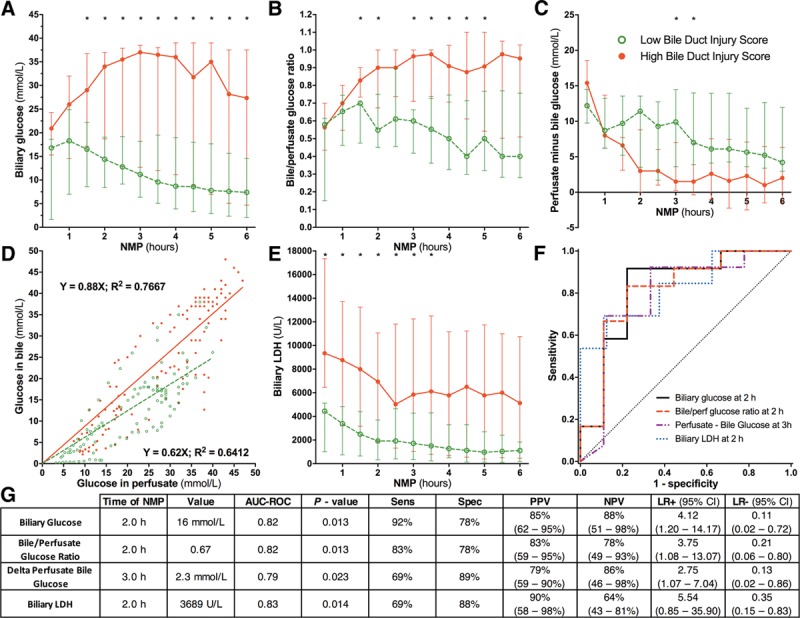
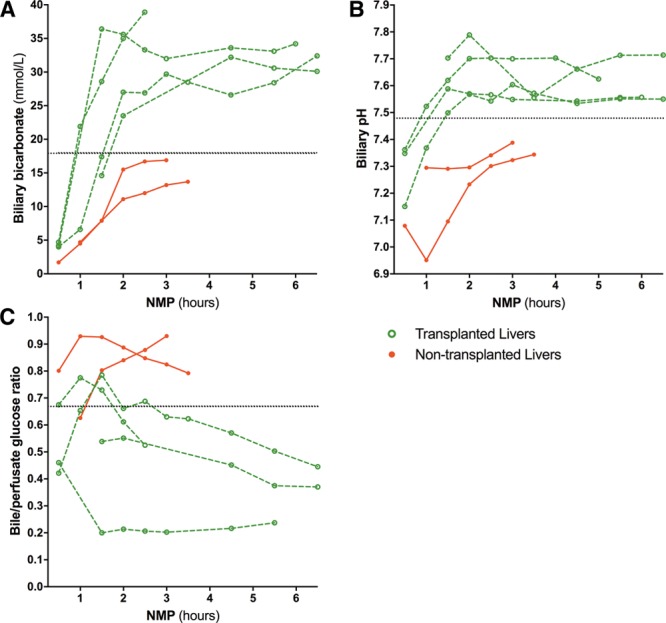
Results: Biliary bicarbonate and pH were significantly higher and biliary glucose was significantly lower in livers with low BDI, compared with high BDI. The following cutoff values were associated with low BDI: biliary bicarbonate greater than 18 mmol/L (P = 0.002), biliary pH greater than 7.48 (P = 0.019), biliary glucose less than 16 mmol/L (P = 0.013), and bile/perfusate glucose ratio less than 0.67 (P = 0.013). In the clinical trial, 4 of 6 livers met these criteria and were transplanted, and none developed clinical evidence of posttransplant cholangiopathy.
Conclusions: Biliary bicarbonate, pH, and glucose during ex situ NMP of liver grafts are accurate biomarkers of BDI and can be easily determined point of care, making them suitable for the pretransplant assessment of bile duct viability. This may improve graft selection and decrease the risk of posttransplant cholangiopathy.
Conflict of interest statement
The authors declare no funding or conflicts of interest.
Figures
Comment in
-
The Authors' Reply to Letter to the Editor, Re: Biliary Bicarbonate, pH, and Glucose Are Suitable Biomarkers of Biliary Viability During Ex Situ Normothermic Machine Perfusion of Human Donor Livers.Transplantation. 2020 Jan;104(1):e41. doi: 10.1097/TP.0000000000002863. Transplantation. 2020. PMID: 31335767 No abstract available.
-
The Authors' Reply: Biliary Bicarbonate, pH, and Glucose Are Suitable Biomarkers of Biliary Viability During Ex Situ Normothermic Machine Perfusion of Human Donor Livers.Transplantation. 2020 Jan;104(1):e40. doi: 10.1097/TP.0000000000002963. Transplantation. 2020. PMID: 31568215 No abstract available.
References
-
- Jochmans I, van Rosmalen M, Pirenne J, et al. Adult liver allocation in Eurotransplant. Transplantation. 2017;101:1542–1550.. - PubMed
-
- de Vries Y, von Meijenfeldt FA, Porte RJ. Post-transplant cholangiopathy: classification, pathogenesis, and preventive strategies. Biochim Biophys Acta Mol Basis Dis. 2018;1864:1507–1515.. - PubMed
-
- Meurisse N, Vanden Bussche S, Jochmans I, et al. Outcomes of liver transplantations using donations after circulatory death: a single-center experience. Transplant Proc. 2012;44:2868–2873.. - PubMed
-
- Jay CL, Lyuksemburg V, Ladner DP, et al. Ischemic cholangiopathy after controlled donation after cardiac death liver transplantation: a meta-analysis. Ann Surg. 2011;253:259–264.. - PubMed
-
- Dubbeld J, Hoekstra H, Farid W, et al. Similar liver transplantation survival with selected cardiac death donors and brain death donors. Br J Surg. 2010;97:744–753.. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
