

Risk of ischemic stroke after discharge from inpatient surgery: Does the type of surgery matter?
- PMID: 30395587
- PMCID: PMC6218083
- DOI: 10.1371/journal.pone.0206990
Risk of ischemic stroke after discharge from inpatient surgery: Does the type of surgery matter?
Abstract
Objective: Stroke is a well-known and devastating complication during the perioperative period. However, detailed stroke risk profiles within 90 days in patients discharged without stroke after inpatient surgery are not fully understood. Using the case-crossover design, we aimed to evaluate the risk of ischemic stroke in these patients.
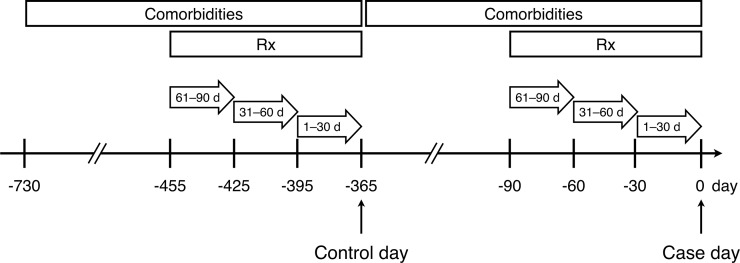
Methods: We included adult patients with the first hospitalization for ischemic stroke between 2011 and 2012 from 23 million enrollees in the National Health Insurance Research Database. Admission date of the hospitalization was defined as the case day and exactly 365 days before the admission date as the control day. The exposure was the last hospitalization for surgery within 1-30, 31-60, or 61-90 days (case period) before the case day or similar time intervals (control period) before the control day. Surgical types were grouped based on the International Classification of Diseases procedure codes. We performed conditional logistic regression adjusting for time-varying variables to determine the relationship between surgery and subsequent stroke, and case-time-control analyses to examine whether the results were confounded by the time-trend in surgery.
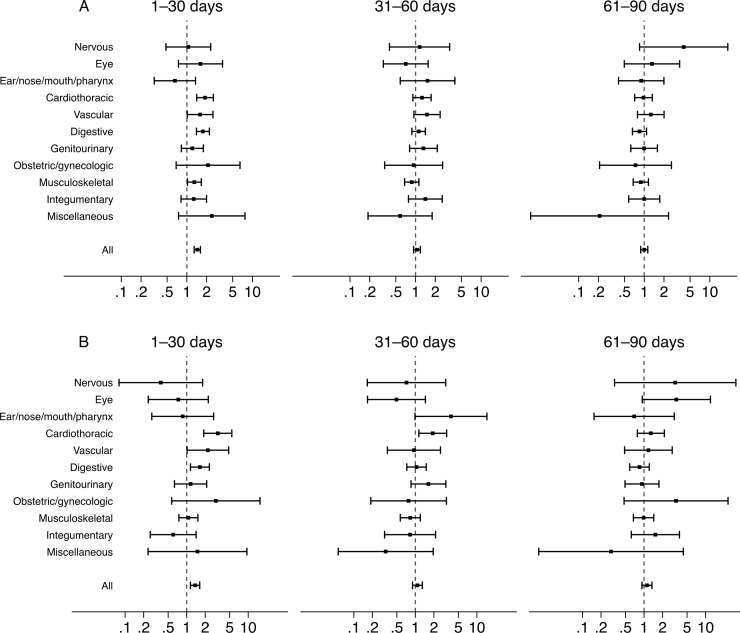
Results: A total of 56596 adult patients (41% female, mean age 69 years) comprised the study population. After adjustment was made for confounding variables, an association between stroke and prior inpatient surgery within 30 days was observed (adjusted odds ratio 1.44; 95% confidence interval 1.29-1.61). Cardiothoracic, vascular, digestive surgery, and musculoskeletal surgery within 30 days independently predicted ischemic stroke in the case-crossover analysis. In the case-time-control analysis, inpatient surgery remained an independent risk factor for ischemic stroke, whereas only cardiothoracic, vascular, and digestive surgery independently predicted ischemic stroke.
Conclusions: Surgery as a whole independently increased the risk of ischemic stroke within 30 days. Among various types of surgery, cardiothoracic, vascular, and digestive surgery significantly increased the risk of ischemic stroke.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Mashour GA, Moore LE, Lele AV, Robicsek SA, Gelb AW. Perioperative care of patients at high risk for stroke during or after non-cardiac, non-neurologic surgery: consensus statement from the Society for Neuroscience in Anesthesiology and Critical Care*. J Neurosurg Anesthesiol. 2014;26: 273–285. 10.1097/ANA.0000000000000087 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
