

Angiotensin II-induced hypertension in rats is only transiently accompanied by lower renal oxygenation
- PMID: 30397212
- PMCID: PMC6218546
- DOI: 10.1038/s41598-018-34211-2
Angiotensin II-induced hypertension in rats is only transiently accompanied by lower renal oxygenation
Abstract
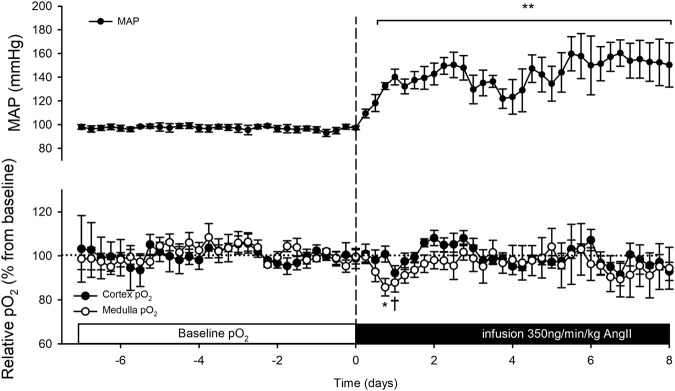
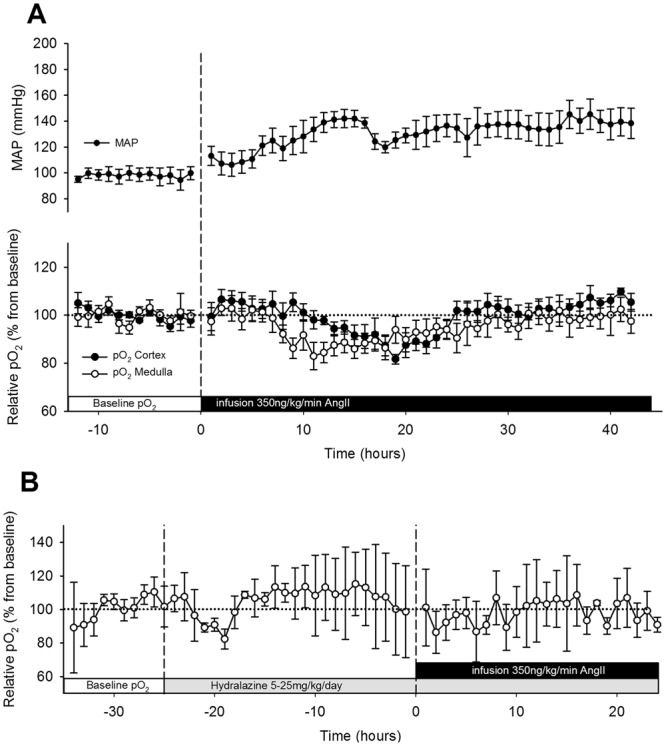
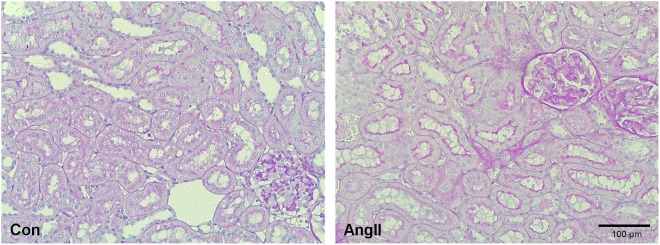
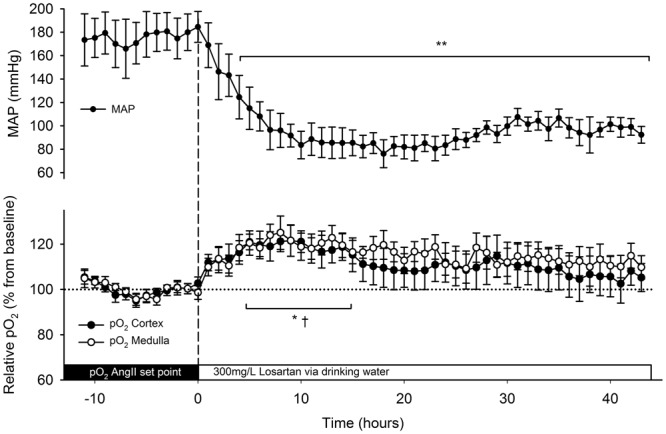
Activation of the renin-angiotensin system may initiate chronic kidney disease. We hypothesised that renal hypoxia is a consequence of hemodynamic changes induced by angiotensin II and occurs prior to development of severe renal damage. Male Sprague-Dawley rats were infused continuously with angiotensin II (350 ng/kg/min) for 8 days. Mean arterial pressure (n = 5), cortical (n = 6) and medullary (n = 7) oxygenation (pO2) were continuously recorded by telemetry and renal tissue injury was scored. Angiotensin II increased arterial pressure gradually to 150 ± 18 mmHg. This was associated with transient reduction of oxygen levels in renal cortex (by 18 ± 2%) and medulla (by 17 ± 6%) at 10 ± 2 and 6 ± 1 hours, respectively after starting infusion. Thereafter oxygen levels normalised to pre-infusion levels and were maintained during the remainder of the infusion period. In rats receiving angiotensin II, adding losartan to drinking water (300 mg/L) only induced transient increase in renal oxygenation, despite normalisation of arterial pressure. In rats, renal hypoxia is only a transient phenomenon during initiation of angiotensin II-induced hypertension.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Fine LG, Orphanides C, Norman JT. Progressive renal disease: the chronic hypoxia hypothesis. Kidney Int Suppl. 1998;65:S74–78. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
