

Acute exacerbation of idiopathic pulmonary fibrosis: a 10-year single-centre retrospective study
- PMID: 30397488
- PMCID: PMC6203000
- DOI: 10.1136/bmjresp-2018-000342
Acute exacerbation of idiopathic pulmonary fibrosis: a 10-year single-centre retrospective study
Abstract
Introduction: In 2016, an international working group proposed a revised definition and new diagnostic criteria for the acute exacerbation of idiopathic pulmonary fibrosis (AE-IPF). Based on these criteria, AE-IPF was diagnosed regardless of the presence or absence of a known trigger and categorised as triggered (T-AE) or idiopathic (I-AE) AE-IPF. However, the clinical characteristics of the newly defined AE-IPF and clinical differences between T-AE and I-AE are unresolved.
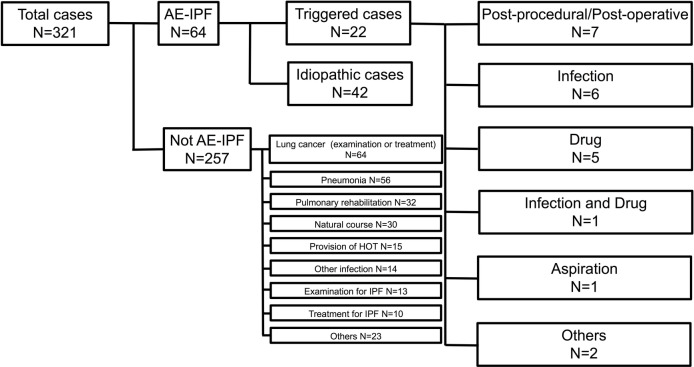
Methods: We retrospectively analysed 64 patients with AE-IPF (I-AE (42), T-AE (22)) admitted to our hospital over a 10- year period.
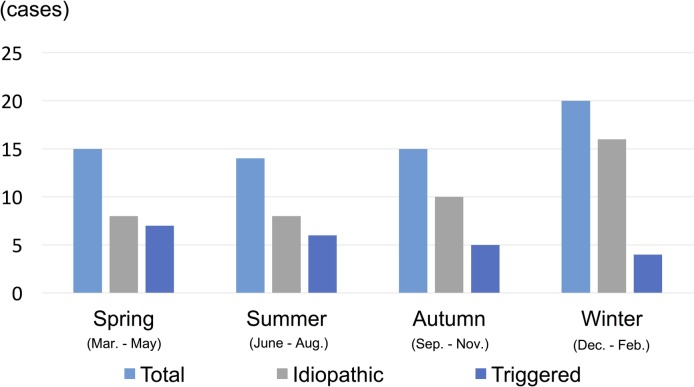
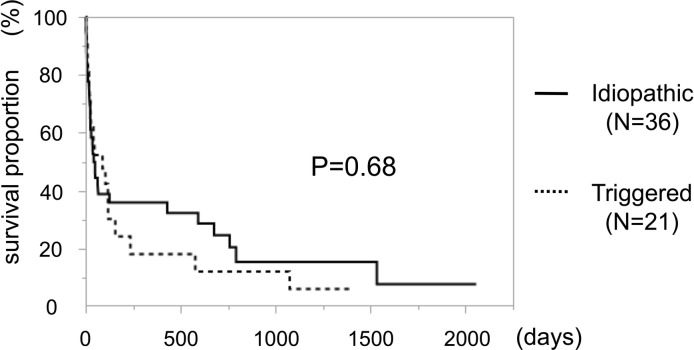
Results: I-AE and T-AE cases did not show differences in in-hospital and long-term outcomes (in-hospital mortality: I-AE 52.4%, T-AE 59.1%, p=0.61; long-term mortality: p=0.68). In the I-AE group, significantly more patients received corticosteroid therapy before an AE (I-AE 35.7%, T-AE 4.5%; p=0.01). Significantly more patients in the T-AE group had lung cancer (I-AE 7.1%, T-AE 59.1%, p<0.001). I-AE occurred more frequently in winter while T-AE did not show seasonality. The white blood cell (WBC) count and haemoglobin (Hb) level were independent predictors of in-hospital deaths in I-AE (WBC: OR 1.87; 95% CI 1.09 to 4.95, p=0.01; Hb: OR 0.26, 95% CI 0.04 to 0.78, p=0.01) but not T-AE.
Discussion: With the introduction of new criteria for AE-IPF, a retrospective study over a 10-year period showed a lack of prognostic difference between I-AE and T-AE. The WBC count and Hb level predicted in-hospital outcome in I-AE cases.
Keywords: acute exacerbation; idiopathic pulmonary fibrosis; outcome; predictor; seasonality; triggered.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Kondoh Y, Taniguchi H, Kawabata Y, et al. Acute exacerbation in idiopathic pulmonary fibrosis. Analysis of clinical and pathologic findings in three cases. Chest 1993;103:1808–12. - PubMed
LinkOut - more resources
Full Text Sources