

Validation of Apolipoprotein A-1 and Fibronectin Fragments as Markers of Parasitological Cure for Congenital Chagas Disease in Children Treated With Benznidazole
- PMID: 30397621
- PMCID: PMC6210386
- DOI: 10.1093/ofid/ofy236
Validation of Apolipoprotein A-1 and Fibronectin Fragments as Markers of Parasitological Cure for Congenital Chagas Disease in Children Treated With Benznidazole
Abstract
Background: No reliable tests or validated biomarkers exist to ensure parasitological cure following treatment of Chagas disease (CD) patients chronically infected with Trypanosoma cruzi. As seroreversion, the only marker of cure, happens more quickly in children, we investigated the correlation between previously identified biomarkers and seroreversion in children.
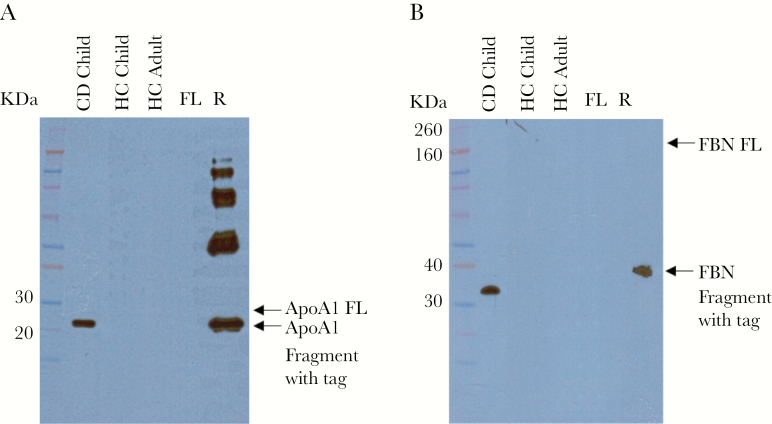
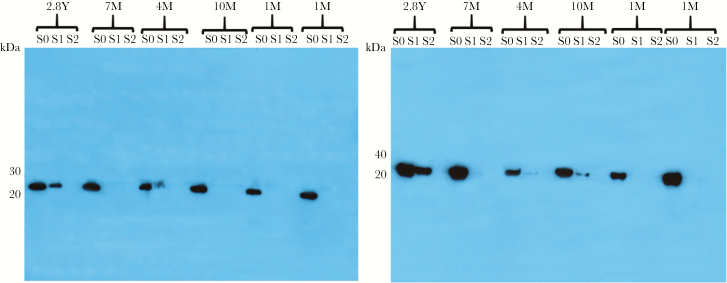
Methods: Thirty CD children (age 1 month to 10 years) diagnosed as T. cruzi positive (time point S0) were treated with benznidazole (BZ) 5-8 mg/kg/d for 60 days. At least 2 serological tests were used to evaluate treatment efficacy from the end of treatment (S1) until seroreversion (S2). Thirty children (age 1 month to 10 years) and 15 adults were used as healthy controls (HCs). Immunoblot and a proteomic-based assay were used to validate previously identified fragments of apolipoprotein A-1 (ApoA1) and fibronectin (FBN) as CD biomarkers.
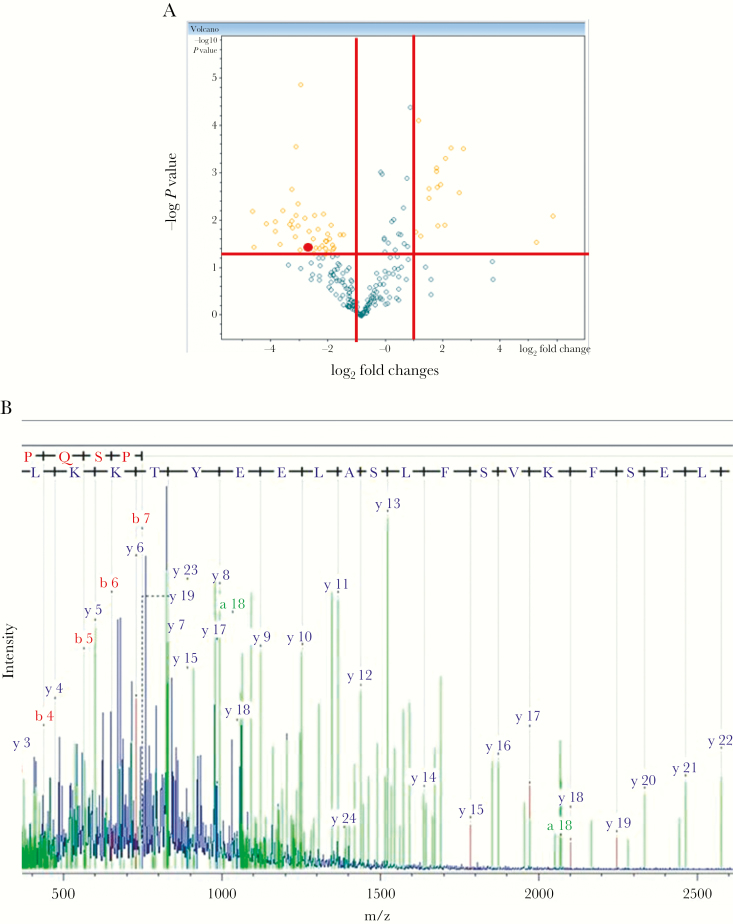
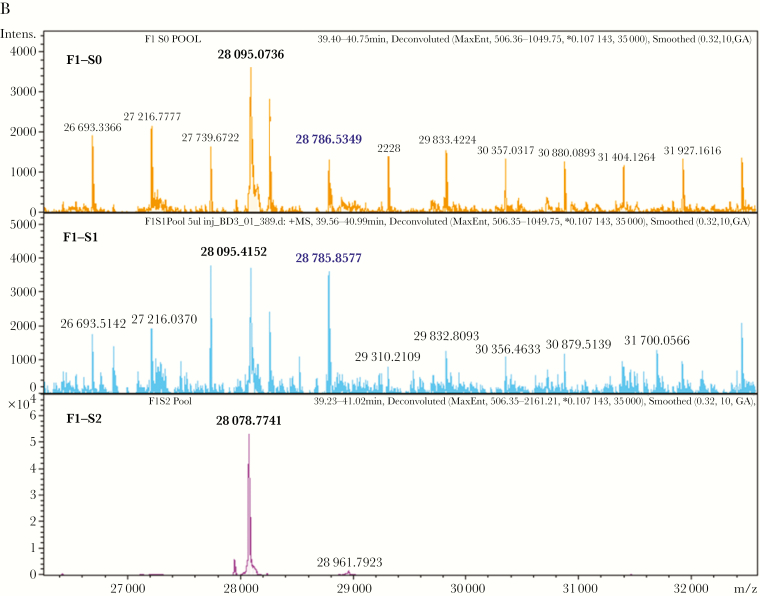
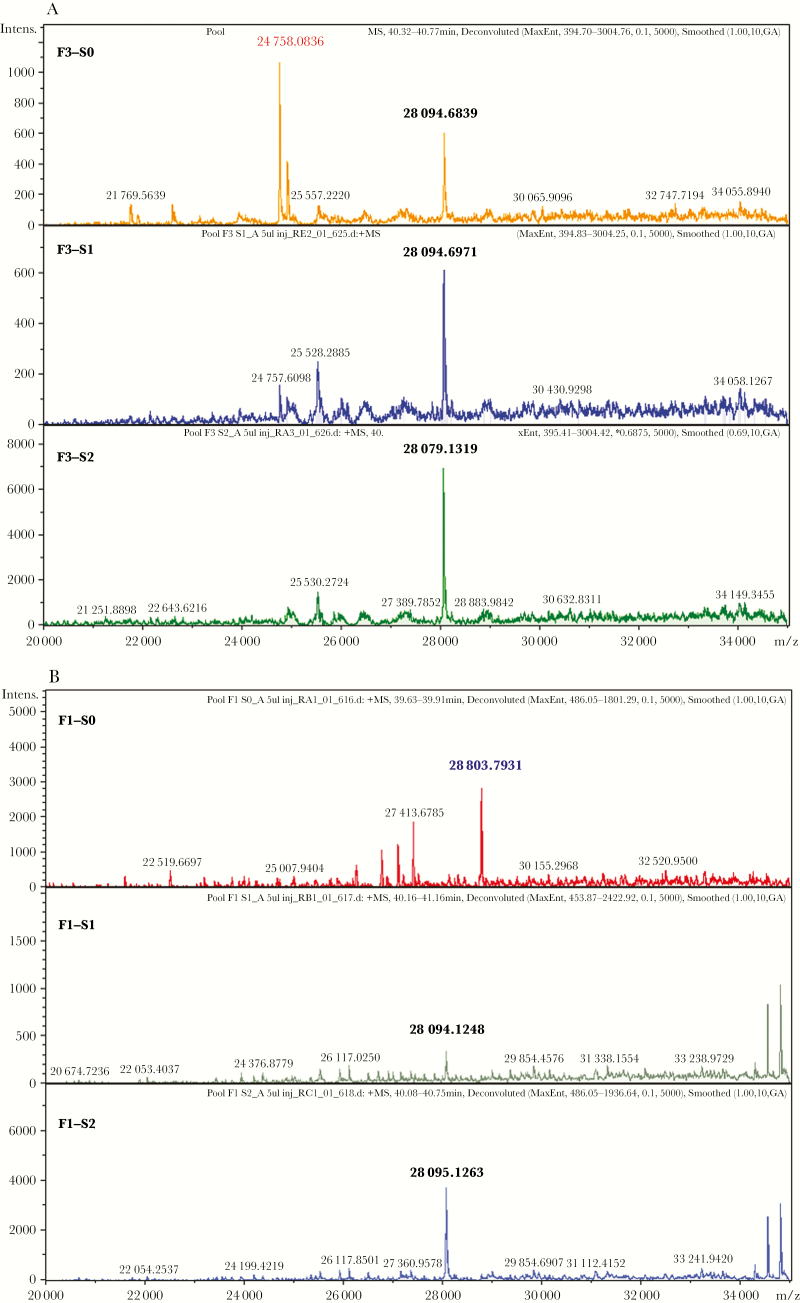
Results: Correlation between seroreversion and absence of ApoA1 and FBN fragments by immunoblot was observed in 30/30 (100%) and 29/30 (96.6%) CD children, respectively. ApoA1 and FBN fragments were absent at the end of BZ treatment in 20/30 (66.6%) and 16/30 (53.3%) children, respectively. Absence of fragments in serum profiles was confirmed by mass spectrometry. Using intact protein analysis, a 28 109-Da protein identified as full-length ApoA1 by tandem mass spectrometry was detected in HC serum samples.
Conclusions: These data confirm that ApoA1 and FBN fragments can discriminate between healthy and T. cruzi-infected samples. Correlation with seroreversion was shown for the first time; results suggest predictive capacity potentially superior to serology, making them potentially useful as surrogate biomarkers.
Keywords: Chagas disease; apolipoprotein A-1; biomarkers; children; fibronectin; test of cure.
Figures

Similar articles
-
Prediction of parasitological cure in children infected with Trypanosoma cruzi using a novel multiplex serological approach: an observational, retrospective cohort study.Lancet Infect Dis. 2021 Aug;21(8):1141-1150. doi: 10.1016/S1473-3099(20)30729-5. Epub 2021 Apr 6. Lancet Infect Dis. 2021. PMID: 33836157
-
Apolipoprotein A1 and Fibronectin Fragments as Markers of Cure for the Chagas Disease.Methods Mol Biol. 2019;1955:263-273. doi: 10.1007/978-1-4939-9148-8_20. Methods Mol Biol. 2019. PMID: 30868534
-
Serum biomarkers predictive of cure in Chagas disease patients after nifurtimox treatment.BMC Infect Dis. 2014 Jun 3;14:302. doi: 10.1186/1471-2334-14-302. BMC Infect Dis. 2014. PMID: 24894358 Free PMC article.
-
Identification of novel diagnostic serum biomarkers for Chagas' disease in asymptomatic subjects by mass spectrometric profiling.J Clin Microbiol. 2010 Apr;48(4):1139-49. doi: 10.1128/JCM.02207-09. Epub 2010 Jan 13. J Clin Microbiol. 2010. PMID: 20071547 Free PMC article.
-
Role of nucleic acid amplification assays in monitoring treatment response in chagas disease: Usefulness in clinical trials.Acta Trop. 2019 Nov;199:105120. doi: 10.1016/j.actatropica.2019.105120. Epub 2019 Jul 31. Acta Trop. 2019. PMID: 31376368 Review.
Cited by
-
New metabolic signature for Chagas disease reveals sex steroid perturbation in humans and mice.Heliyon. 2022 Dec 15;8(12):e12380. doi: 10.1016/j.heliyon.2022.e12380. eCollection 2022 Dec. Heliyon. 2022. PMID: 36590505 Free PMC article.
-
Intra-host Trypanosoma cruzi strain dynamics shape disease progression: the missing link in Chagas disease pathogenesis.Microbiol Spectr. 2023 Sep 5;11(5):e0423622. doi: 10.1128/spectrum.04236-22. Online ahead of print. Microbiol Spectr. 2023. PMID: 37668388 Free PMC article.
-
Defeating the trypanosomatid trio: proteomics of the protozoan parasites causing neglected tropical diseases.RSC Med Chem. 2020 May 22;11(6):625-645. doi: 10.1039/d0md00122h. eCollection 2020 Jun 1. RSC Med Chem. 2020. PMID: 33479664 Free PMC article. Review.
-
Fibronectin degradation as biomarker for Trypanosoma cruzi infection and treatment monitoring in mice.Parasitology. 2021 Aug;148(9):1067-1073. doi: 10.1017/S0031182021000809. Epub 2021 May 24. Parasitology. 2021. PMID: 34024298 Free PMC article.
References
-
- Stanaway JD, Roth G. The burden of Chagas disease: estimates and challenges. Glob Heart 2015; 10:139–44. - PubMed
-
- Pérez-Molina JA, Perez AM, Norman FF, et al. . Old and new challenges in Chagas disease. Lancet Infect Dis 2015; 15:1347–56. - PubMed
-
- WHO. Chagas disease. www.who.int/mediacentre/factsheets/fs340/en/. Accessed March 2017.
-
- Muñoz J, Coll O, Juncosa T, et al. . Prevalence and vertical transmission of Trypanosoma cruzi infection among pregnant Latin American women attending 2 maternity clinics in Barcelona, Spain. Clin Infect Dis 2009; 48:1736–40. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
