

Identification of Aberrant Muscle Bellies in the Carpal Tunnel using Sonography
- PMID: 30397686
- PMCID: PMC6214479
- DOI: 10.1177/8756479318807469
Identification of Aberrant Muscle Bellies in the Carpal Tunnel using Sonography
Abstract
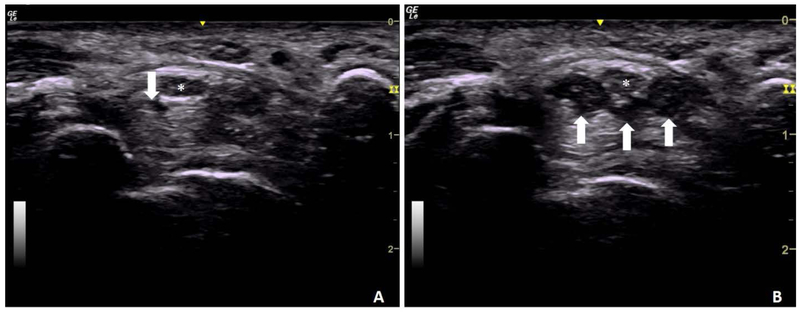
Musculoskeletal sonography is being widely used for evaluation of structures within the carpal tunnel. While some anatomical variants, such as bifurcated median nerves and persistent median arteries, have been well documented, limited literature describes the sonographic appearance of aberrant muscle bellies within the carpal tunnel. Multiple examples of the sonographic appearance of flexor digitorum superficialis and lumbrical muscle bellies extending into the carpal tunnel are provided. Techniques for static image acquisition and analysis are discussed, and the use of dynamic imaging to confirm which specific muscle belly is involved is described. Knowledge of the potential presence of muscle bellies in these images and ability to identify these structures is vital to avoid misclassification or misdiagnosis as abnormal pathology. The case examples are situated among current published evidence regarding how such anomalies may be related to the development of pathologies, such as carpal tunnel syndrome.
Keywords: Carpal tunnel; aberrant muscle; musculoskeletal sonography.
Figures




Similar articles
-
Elongated muscle belly of the flexor digitorum superficial causing carpal tunnel syndrome.Hand (N Y). 2012 Sep;7(3):333-4. doi: 10.1007/s11552-012-9435-z. Hand (N Y). 2012. PMID: 23997744 Free PMC article.
-
Anomalous Flexor Digitorum Superficialis Muscle Belly Associated with Carpal Tunnel Syndrome.J Hand Surg Glob Online. 2023 May 8;5(4):471-473. doi: 10.1016/j.jhsg.2023.04.007. eCollection 2023 Jul. J Hand Surg Glob Online. 2023. PMID: 37521556 Free PMC article.
-
Recurrent carpal tunnel syndrome associated with extension of flexor digitorum muscle bellies into the carpal tunnel: A case series.Arch Plast Surg. 2018 Sep;45(5):474-478. doi: 10.5999/aps.2017.00724. Epub 2018 Sep 15. Arch Plast Surg. 2018. PMID: 30282420 Free PMC article.
-
Bilateral flexor digitorum superficialis brevis of the little finger: a rare cause of carpal tunnel syndrome.Hand Surg Rehabil. 2021 Oct;40(5):682-686. doi: 10.1016/j.hansur.2021.05.003. Epub 2021 May 15. Hand Surg Rehabil. 2021. PMID: 34004370 Review.
-
Accessory Hand Muscles Over the Transverse Carpal Ligament: An Obstacle in Carpal Tunnel Surgery.World Neurosurg. 2023 Feb;170:e402-e415. doi: 10.1016/j.wneu.2022.11.045. Epub 2022 Nov 12. World Neurosurg. 2023. PMID: 36379360
Cited by
-
Clinical, Electrophysiological, and Intraoperative Analysis and Postoperative Success of Revision Surgery for Persistent and Recurrent Carpal Tunnel Syndrome.Eplasty. 2024 Oct 17;24:e56. eCollection 2024. Eplasty. 2024. PMID: 39474004 Free PMC article.
References
-
- Roll SC, Evans KD. Sonographic Representation of Bifid Median Nerve and Persistent Median Artery. Journal of Diagnostic Medical Sonography. 2011;27(2):89–94.
Grants and funding
LinkOut - more resources
Full Text Sources