

Natural Progression of Symptom Change and Recovery From Concussion in a Pediatric Population
- PMID: 30398522
- PMCID: PMC6583432
- DOI: 10.1001/jamapediatrics.2018.3820
Natural Progression of Symptom Change and Recovery From Concussion in a Pediatric Population
Abstract
Importance: The natural progression of symptom change and recovery remains poorly defined in children after concussion.
Objectives: To describe the natural progression of symptom change by age group (5-7, 8-12, and 13-18 years) and sex, as well as to develop centile curves to inform families about children after injury recovery.
Design, setting, and participants: Planned secondary analysis of a prospective multicenter cohort study (Predicting Persistent Postconcussive Problems in Pediatrics). The setting was 9 pediatric emergency departments within the Pediatric Emergency Research Canada (PERC) network. Participants were aged 5 to 18 years with acute concussion, enrolled from August 1, 2013, to May 31, 2015, and data analyses were performed between January 2018 and March 2018.
Exposures: Participants had a concussion consistent with the Zurich Consensus Statement on Concussion in Sport diagnostic criteria and 85% completeness of the Postconcussion Symptom Inventory (PCSI) at each time point.
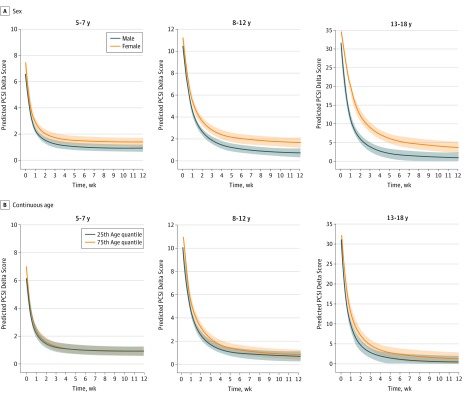
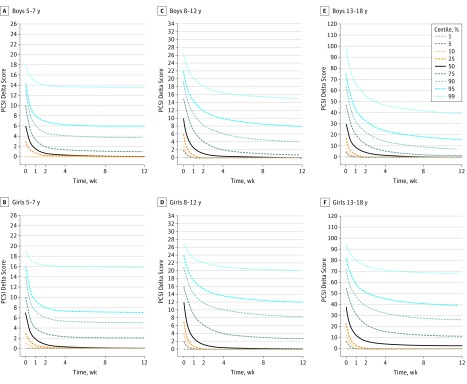
Main outcomes and measures: The primary outcome was symptom change, defined as current rating minus preinjury rating (delta score), at presentation and 1, 2, 4, 8, and 12 weeks after injury, measured using the PCSI. Symptoms were self-rated for ages 8 to 18 years and rated by the child and parent for ages 5 to 7 years. The secondary outcome was recovery, defined as no change in symptoms relative to current preinjury PCSI ratings (delta score = 0). Mixed-effects models incorporated the total score, adjusting for random effects (site and participant variability), fixed-effects indicators (age, sex, time, age by time interaction, and sex by time interaction), and variables associated with recovery. Recovery centile curves by age and sex were computed.
Results: A total of 3063 children (median age, 12.0 years [interquartile range, 9.2-14.6 years]; 60.7% male) completed the primary outcome; 2716 were included in the primary outcome analysis. For the group aged 5 to 7 years, symptom change primarily occurred the first week after injury; by 2 weeks, 75.6% of symptoms had improved (PCSI change between 0 and 2 weeks, -5.3; 95% CI, -5.5 to -5.0). For the groups aged 8 to 12 years and 13 to 18 years, symptom change was prominent the first 2 weeks but flattened between 2 and 4 weeks. By 4 weeks, 83.6% and 86.2% of symptoms, respectively, had improved for the groups aged 8 to 12 years (PCSI change between 0 and 4 weeks, -9.0; 95% CI, -9.6 to -8.4) and 13 to 18 years (PCSI change between 0 and 4 weeks, -28.6; 95% CI, -30.8 to -26.3). Sex by time interaction was significant only for the adolescent group (β = 0.32; 95% CI, 0.21-0.43; P < .001). Most adolescent girls had not recovered by week 12.
Conclusions and relevance: Symptom improvement primarily occurs in the first 2 weeks after concussion in children and in the first 4 weeks after concussion in preadolescents and male adolescents. Female adolescents appear to have protracted recovery. The derived recovery curves may be useful for evidence-based anticipatory guidance.
Conflict of interest statement
Figures
References
-
- Novak Z, Aglipay M, Barrowman N, et al. ; Pediatric Emergency Research Canada Predicting Persistent Postconcussive Problems in Pediatrics (PERC 5P) Concussion Team . Association of persistent postconcussion symptoms with pediatric quality of life. JAMA Pediatr. 2016;170(12):. doi: 10.1001/jamapediatrics.2016.2900 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
