

Editorial
doi: 10.1530/EC-18-0398.
Immunotherapy failure in adrenocortical cancer: where next?
Affiliations
- PMID: 30400026
- PMCID: PMC6280582
- DOI: 10.1530/EC-18-0398
Item in Clipboard
Editorial
Immunotherapy failure in adrenocortical cancer: where next?
Endocr Connect.
2018 Dec.
Abstract
Immunotherapy is widely used in the treatment of different cancer types, including metastatic melanoma, non-small cell lung cancer, renal cell carcinoma and urothelial cancer. The results of the phase I JAVELIN study failed to demonstrate a substantial activity of the PDL-1 inhibitor Avelumab in advanced adrenocortical carcinoma (ACC). This editorial focus on the possible mechanisms of ACC immunoevasion and suggests strategies to overcome the intrinsic immunotherapy resistance of this disease.
Figures
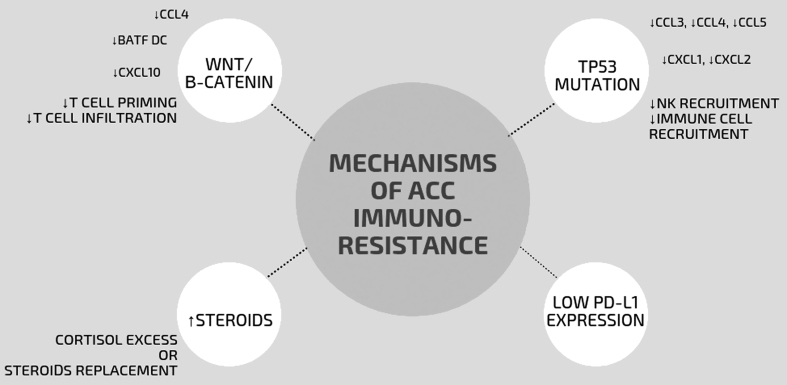
Mechanisms of ACC immunoresistance. The upregulation of β-catenin reduces production of different chemokines (such as CCL4, BATF Dcs, CXCL10) leading to the lack of T cell priming and the consequent recruitment of effector T cells in the tumor. TP53‐mutated tumor cells lack production of key chemokines required for the recruitment of natural killer cells and T cells, which results in exclusion of effector T cell from the tumor infiltration. Low PD-L1 expression and increased production of steroids can impair tumor immunogenicity. BATF DC, basic leucine zipper transcriptional factor ATF-like 3 lineage dendritic cells; CCL, CC-chemokine ligand; CXCL, CXC-chemokine ligand; PD-L1, programmed cell death 1 ligand 1.
References
-
- Fassnacht M, Dekkers O, Else T, Baudin E, Berruti A, de Krijger RR, Haak HR, Mihai R, Assie G, Terzolo M. European Society of Endocrinology Clinical Practice Guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the European Network for the Study of Adrenal Tumors. European Journal of Endocrinology 2018. 179 G1–G46. (10.1530/EJE-18-0608) - DOI - PubMed
-
- Amin A, White RL., Jr High-dose interleukin-2: is it still indicated for melanoma and RCC in an era of targeted therapies? Oncology 2013. 27 680–691. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
