

Combination Therapy with Oseltamivir and Favipiravir Delays Mortality but Does Not Prevent Oseltamivir Resistance in Immunodeficient Mice Infected with Pandemic A(H1N1) Influenza Virus
- PMID: 30400276
- PMCID: PMC6266789
- DOI: 10.3390/v10110610
Combination Therapy with Oseltamivir and Favipiravir Delays Mortality but Does Not Prevent Oseltamivir Resistance in Immunodeficient Mice Infected with Pandemic A(H1N1) Influenza Virus
Abstract
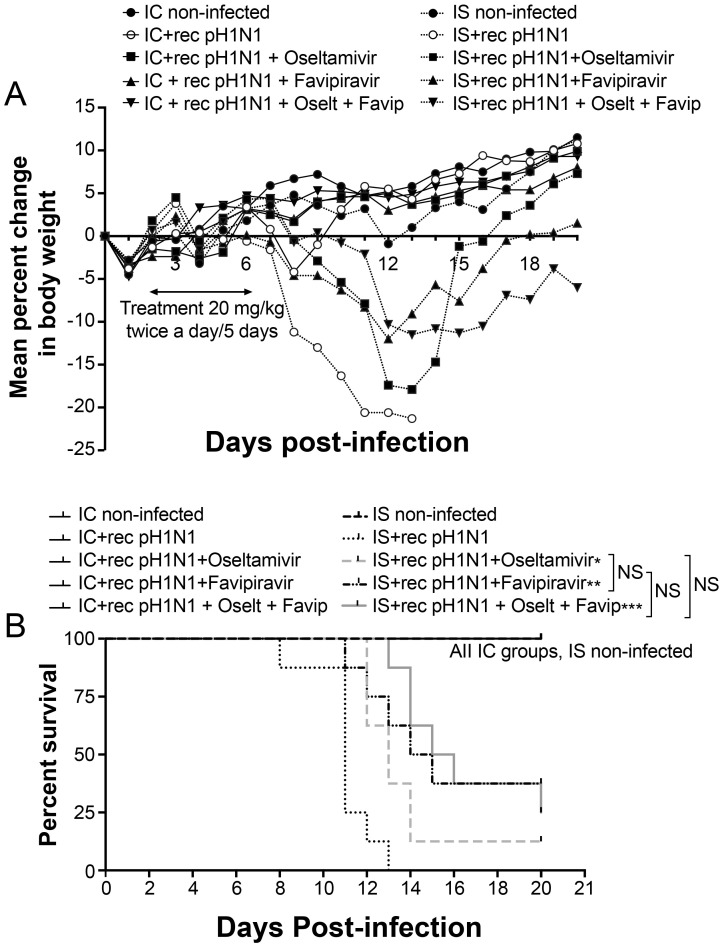
Immunosuppressed individuals can shed influenza virus for prolonged periods of time, leading to the frequent emergence of antiviral resistance. We evaluated the benefits of oseltamivir and favipiravir combination therapy compared to single antiviral agents and monitored the emergence of drug-resistant variants in a pharmacologically immunosuppressed mouse model infected with the A(H1N1) pandemic influenza virus. C57BL/6 mice were immunosuppressed with cyclophosphamide and infected with a lethal dose of pandemic influenza A(H1N1) virus. Forty-eight hours post-infection, mice were treated with oseltamivir (20 mg/kg), favipiravir (20 or 50 mg/kg) or both agents BID for 5 or 10 days. Body weight losses, survival rates, lung viral titers, cytokine levels and emergence of resistant viruses were evaluated. Treatment of immunosuppressed mice with high (50 mg/kg) but not low (20 mg/kg) doses of favipiravir in combination with oseltamivir (20 mg/kg) significantly delayed mortality and reduced lung viral titers compared to treatment with a single drug regimen with oseltamivir but did not prevent the emergence of oseltamivir-resistant H275Y neuraminidase variants. Combination therapy with oseltamivir and favipiravir should be considered for evaluation in clinical trials.
Keywords: combination therapy; favipiravir; immunosuppression; mice; oseltamivir; pandemic influenza virus; resistance.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




Similar articles
-
In vitro activity of favipiravir and neuraminidase inhibitor combinations against oseltamivir-sensitive and oseltamivir-resistant pandemic influenza A (H1N1) virus.Arch Virol. 2014 Jun;159(6):1279-91. doi: 10.1007/s00705-013-1922-1. Epub 2013 Dec 6. Arch Virol. 2014. PMID: 24311151
-
Combination effects of peramivir and favipiravir against oseltamivir-resistant 2009 pandemic influenza A(H1N1) infection in mice.PLoS One. 2014 Jul 3;9(7):e101325. doi: 10.1371/journal.pone.0101325. eCollection 2014. PLoS One. 2014. PMID: 24992479 Free PMC article.
-
Combination Therapy With Neuraminidase and Polymerase Inhibitors in Nude Mice Infected With Influenza Virus.J Infect Dis. 2018 Mar 5;217(6):887-896. doi: 10.1093/infdis/jix606. J Infect Dis. 2018. PMID: 29186472 Free PMC article.
-
Emerging oseltamivir resistance in seasonal and pandemic influenza A/H1N1.J Clin Virol. 2011 Oct;52(2):70-8. doi: 10.1016/j.jcv.2011.05.019. Epub 2011 Jun 17. J Clin Virol. 2011. PMID: 21684202 Review.
-
[Favipiravir, a new concept of antiviral drug against influenza viruses].Rev Esp Quimioter. 2017 Apr;30(2):79-83. Epub 2017 Feb 8. Rev Esp Quimioter. 2017. PMID: 28176519 Review. Spanish.
Cited by
-
In Vitro Combinations of Baloxavir Acid and Other Inhibitors against Seasonal Influenza A Viruses.Viruses. 2020 Oct 8;12(10):1139. doi: 10.3390/v12101139. Viruses. 2020. PMID: 33049959 Free PMC article.
-
Synergistic PA and HA mutations confer mouse adaptation of a contemporary A/H3N2 influenza virus.Sci Rep. 2019 Nov 12;9(1):16616. doi: 10.1038/s41598-019-51877-4. Sci Rep. 2019. PMID: 31719554 Free PMC article.
-
Baloxavir Marboxil Treatment of Nude Mice Infected With Influenza A Virus.J Infect Dis. 2020 Apr 27;221(10):1699-1702. doi: 10.1093/infdis/jiz665. J Infect Dis. 2020. PMID: 31837268 Free PMC article.
-
Repurposing approved drugs on the pathway to novel therapies.Med Res Rev. 2020 Mar;40(2):586-605. doi: 10.1002/med.21627. Epub 2019 Aug 20. Med Res Rev. 2020. PMID: 31432544 Free PMC article. Review.
-
Baloxavir marboxil, a novel cap-dependent endonuclease inhibitor potently suppresses influenza virus replication and represents therapeutic effects in both immunocompetent and immunocompromised mouse models.PLoS One. 2019 May 20;14(5):e0217307. doi: 10.1371/journal.pone.0217307. eCollection 2019. PLoS One. 2019. PMID: 31107922 Free PMC article.
References
-
- Khanna N., Steffen I., Studt J.D., Schreiber A., Lehmann T., Weisser M., Fluckiger U., Gratwohl A., Halter J., Hirsch H.H. Outcome of influenza infections in outpatients after allogeneic hematopoietic stem cell transplantation. Transpl. Infect. Dis. 2009;11:100–105. doi: 10.1111/j.1399-3062.2008.00362.x. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
