

Maternal β-Cell Adaptations in Pregnancy and Placental Signalling: Implications for Gestational Diabetes
- PMID: 30400566
- PMCID: PMC6274918
- DOI: 10.3390/ijms19113467
Maternal β-Cell Adaptations in Pregnancy and Placental Signalling: Implications for Gestational Diabetes
Abstract
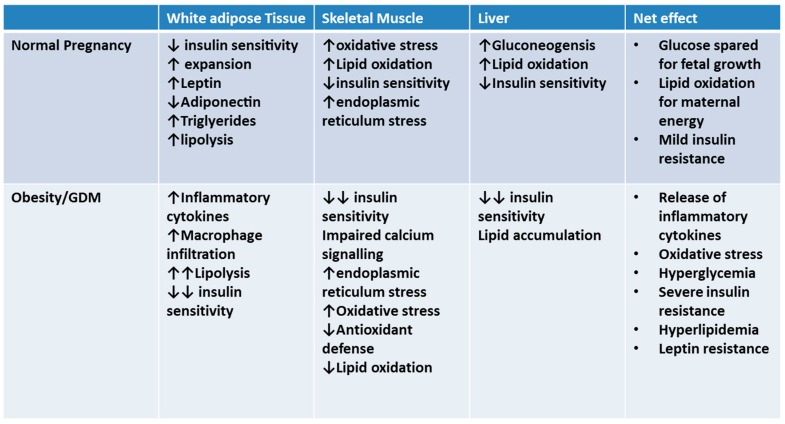
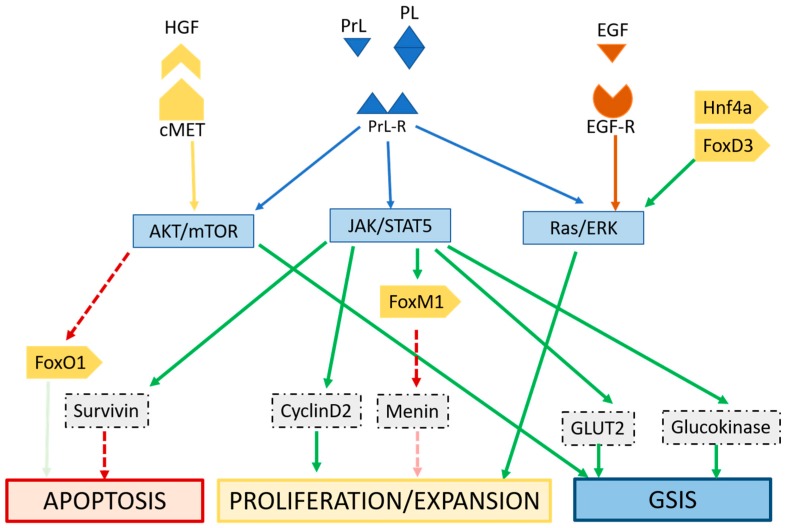
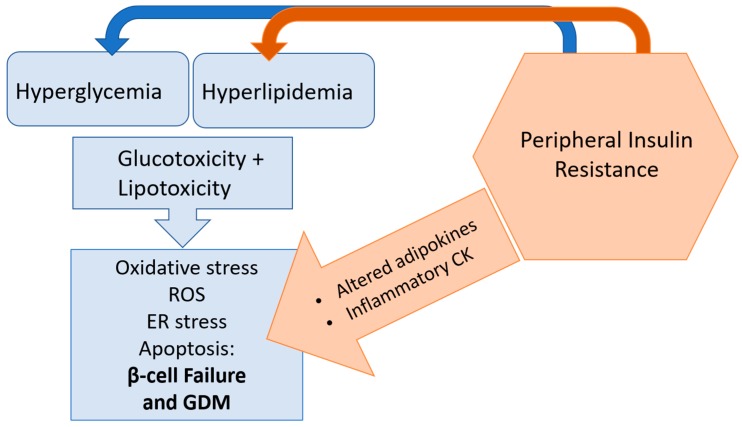
Rates of gestational diabetes mellitus (GDM) are on the rise worldwide, and the number of pregnancies impacted by GDM and resulting complications are also increasing. Pregnancy is a period of unique metabolic plasticity, during which mild insulin resistance is a physiological adaptation to prioritize fetal growth. To compensate for this, the pancreatic β-cell utilizes a variety of adaptive mechanisms, including increasing mass, number and insulin-secretory capacity to maintain glucose homeostasis. When insufficient insulin production does not overcome insulin resistance, hyperglycemia can occur. Changes in the maternal system that occur in GDM such as lipotoxicity, inflammation and oxidative stress, as well as impairments in adipokine and placental signalling, are associated with impaired β-cell adaptation. Understanding these pathways, as well as mechanisms of β-cell dysfunction in pregnancy, can identify novel therapeutic targets beyond diet and lifestyle interventions, insulin and antihyperglycemic agents currently used for treating GDM.
Keywords: gestational diabetes mellitus; insulin; placenta; pregnancy; β-cell.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
