

A risk score system to timely manage treatment in Crohn's disease: a cohort study
- PMID: 30400823
- PMCID: PMC6219027
- DOI: 10.1186/s12876-018-0889-5
A risk score system to timely manage treatment in Crohn's disease: a cohort study
Abstract
Background: Clinical severity and intestinal lesions of Crohn's disease (CD) usually progress over time and require a step up adjustment of the therapy either to prevent or to treat complications. The aim of the study was to develop a simple risk scoring system to assess in individual CD patients the risk of disease progression and the need for more intensive treatment and monitoring.
Methods: Prospective cohort study (January 2002-September 2014) including 160 CD patients (93 female, median age 31 years; disease behavior (B)1 25%, B2 55.6%, B3 19.4%; location (L)1 61%, L3 31.9%, L2 6%; L4 0.6%; perianal disease 28.8%) seen at 6-12-month interval. Median follow-up 7.9 years (IQR: 4.3-10.5 years). Poisson models were used to evaluate predictors, at each clinical assessment, of having the following outcomes at the subsequent clinical assessment a) use of steroids; b) start of azathioprine; c) start of anti-TNF-α drugs; d) need of surgery. For each outcome 32 variables, including demographic and clinical characteristics of patients and assessment of CD intestinal lesions and complications, were evaluated as potential predictors. The predictors included in the model were chosen by a backward selection. Risk scores were calculated taking for each predictor the integer part of the Poisson model parameter.
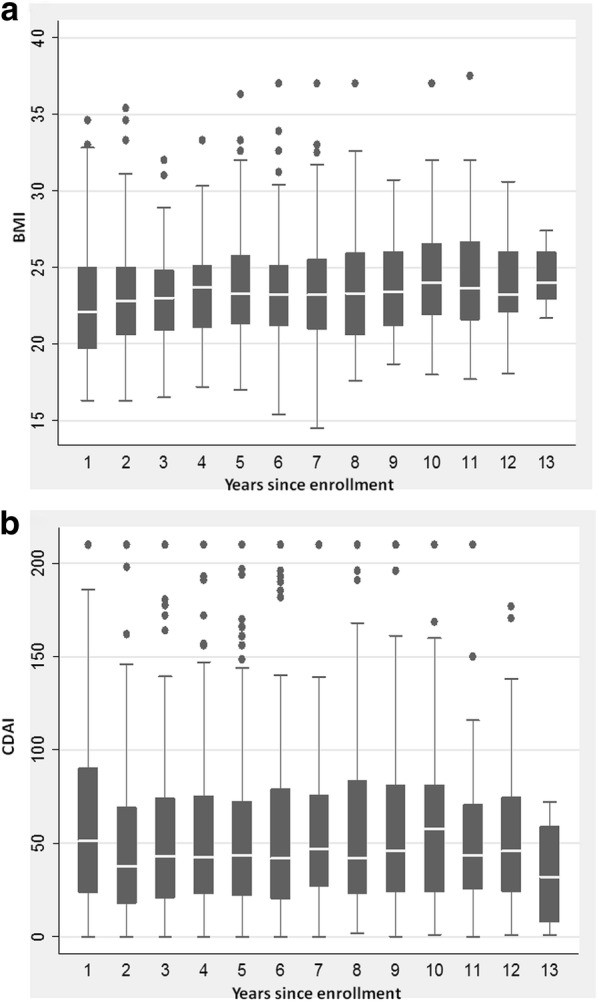
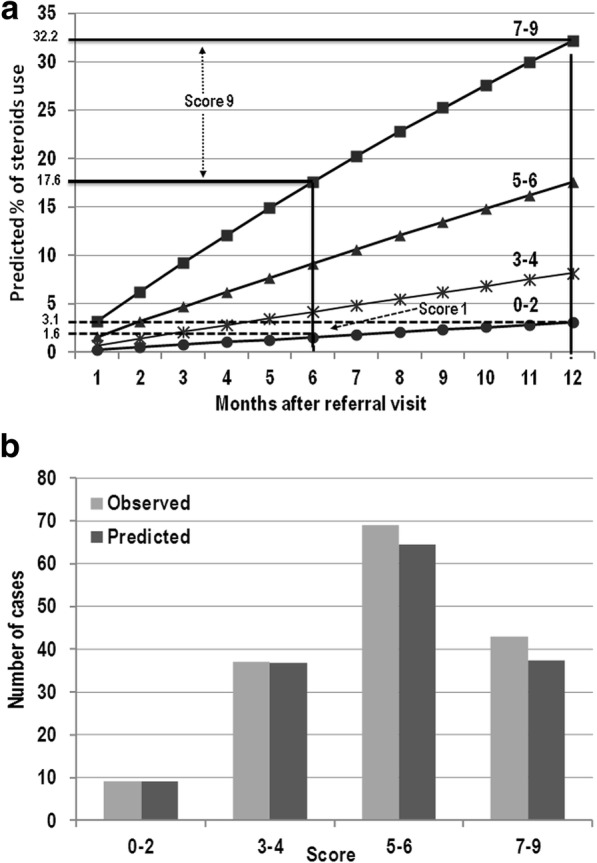
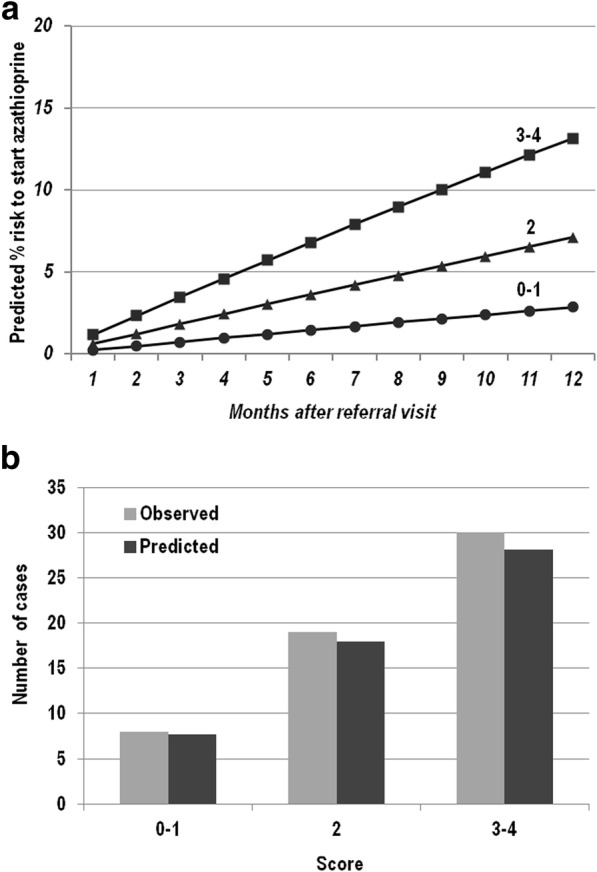
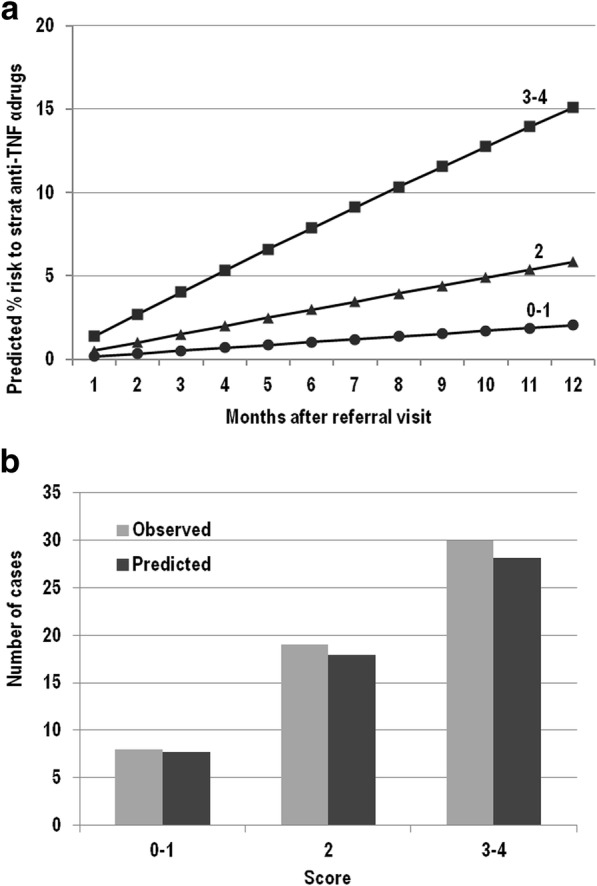
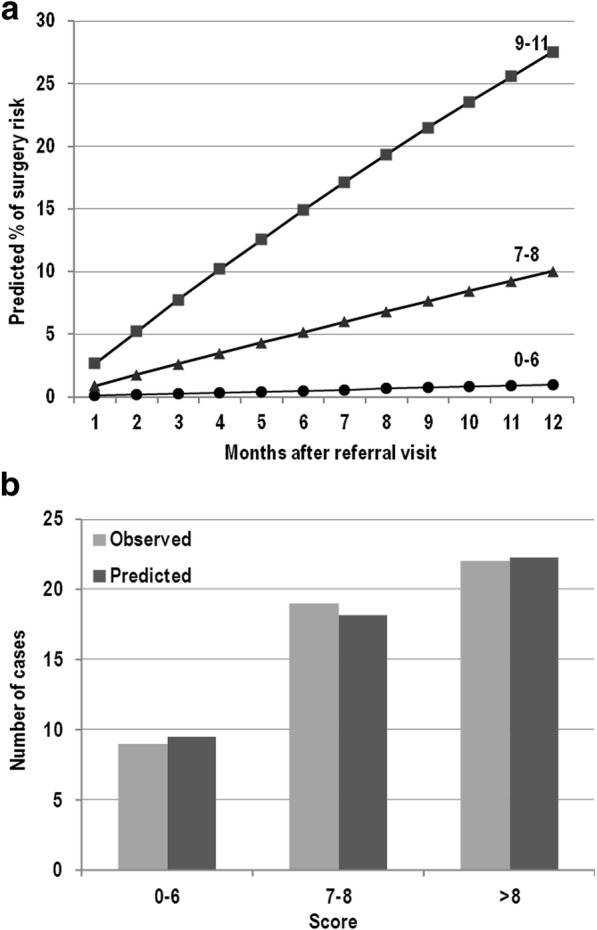
Results: Considering 1464 clinical assessments 12 independent risk factors were identified, CD lesions, age at diagnosis < 40 years, stricturing behavior (B2), specific intestinal symptoms, female gender, BMI < 21, CDAI> 50, presence of inflammatory markers, no previous surgery or presence of termino-terminal anastomosis, current use of corticosteroid, no corticosteroid at first flare-up. Six of these predicted steroids use (score 0-9), three to start azathioprine (score 0-4); three to start anti-TNF-α drugs (score 0-4); six need of surgery (score 0-11). The predicted percentage risk to be treated with surgery within one year since the referral assessment varied from 1 to 28%; with azathioprine from 3 to 13%; with anti-TNF-α drugs from 2 to 15%.
Conclusions: These scores may provide a useful clinical tool for clinicians in the prognostic assessment and treatment adjustment of Crohn's disease in any individual patient.
Keywords: Crohn’s disease; Risk factors, small intestine contrast ultrasonography; Risk score system; Therapy, medical, surgical.
Conflict of interest statement
Ethics approval and consent to participate
Written informed consent was obtained from each subject and the study protocol was approved by the local committee of the Department of Internal Medicine and Medical Specialties University Hospital (Policlinico “Umberto I” viale del Policlinico 155, 00161) Rome, 6 December 2001.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
