

Bone and Soft-Tissue Biopsies: What You Need to Know
- PMID: 30402003
- PMCID: PMC6218252
- DOI: 10.1055/s-0038-1669467
Bone and Soft-Tissue Biopsies: What You Need to Know
Abstract
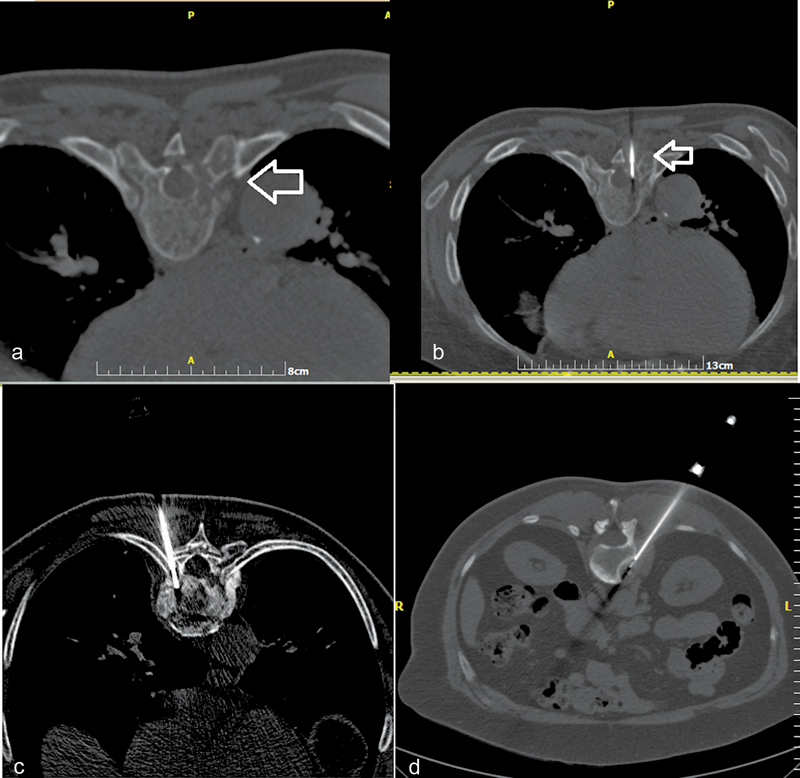
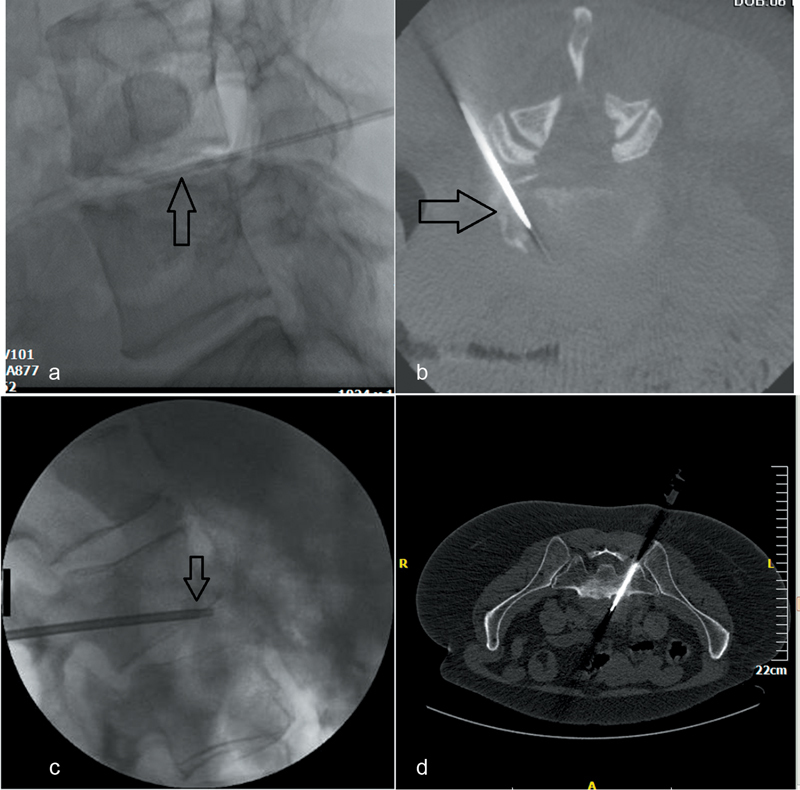
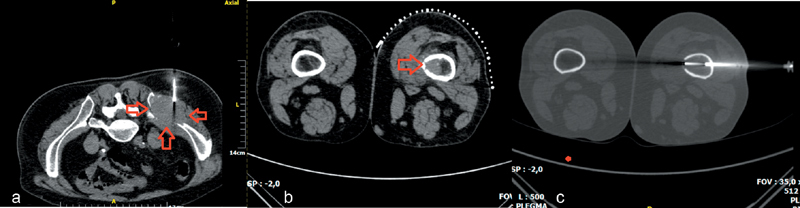
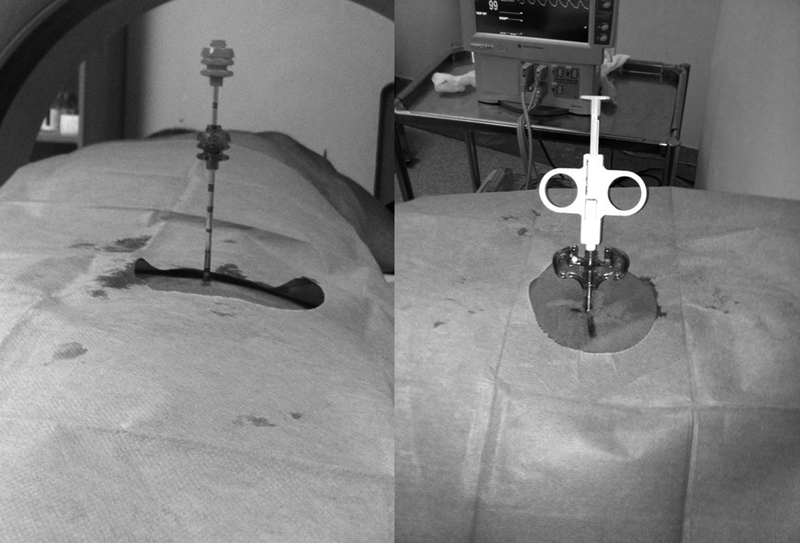
Percutaneous, image-guided musculoskeletal biopsy, due to its minimal invasive nature, when compared with open surgical biopsy, is a safe and effective technique which is widely used in many institutions as the primary method to acquire tissue and bone samples. Indications include histopathologic and molecular assessment of a musculoskeletal lesion, exclusion of malignancy in a bone/vertebral fracture, examination of bone marrow, and infection investigation. Preprocedural workup should include both imaging (for lesion assessment and staging) and laboratory (including coagulation tests and platelet count) studies. In selected cases, antibiotic prophylaxis should be administered before the biopsy. Core needle biopsy of musculoskeletal lesions has a diagnostic accuracy that ranges from 66 to 98% with higher diagnostic yield for lytic, large-size, malignant lesions and when multiple and long specimens are obtained. Reported complication rates range between 0 and 10% and usually do not exceed 5%, with a suggested threshold of 2%. The purpose of this review article is to illustrate the technical aspects, the indications, and the methodology of percutaneous image-guided bone biopsy that will assist the interventional radiologist to perform these minimal invasive techniques.
Keywords: Imaging guidance; interventional radiology; musculoskeletal lesion; percutaneous biopsy.
Conflict of interest statement
Figures
References
-
- Veltri A, Bargellini I, Giorgi L, Almeida P AMS, Akhan O. CIRSE guidelines on percutaneous needle biopsy (PNB) Cardiovasc Intervent Radiol. 2017;40(10):1501–1513. - PubMed
-
- Gogna A, Peh W C, Munk P L.Image-guided musculoskeletal biopsy Radiol Clin North Am 20084603455–473., v - PubMed
-
- Liu B, Limback J, Kendall M et al.Safety of CT-guided bone marrow biopsy in thrombocytopenic patients: a retrospective review. J Vasc Interv Radiol. 2017;28(12):1727–1731. - PubMed
-
- Holmes M G, Foss E, Joseph G et al.CT-guided bone biopsies in metastatic castration-resistant prostate cancer: factors predictive of maximum tumor yield. J Vasc Interv Radiol. 2017;28(08):1073–10810. - PubMed
